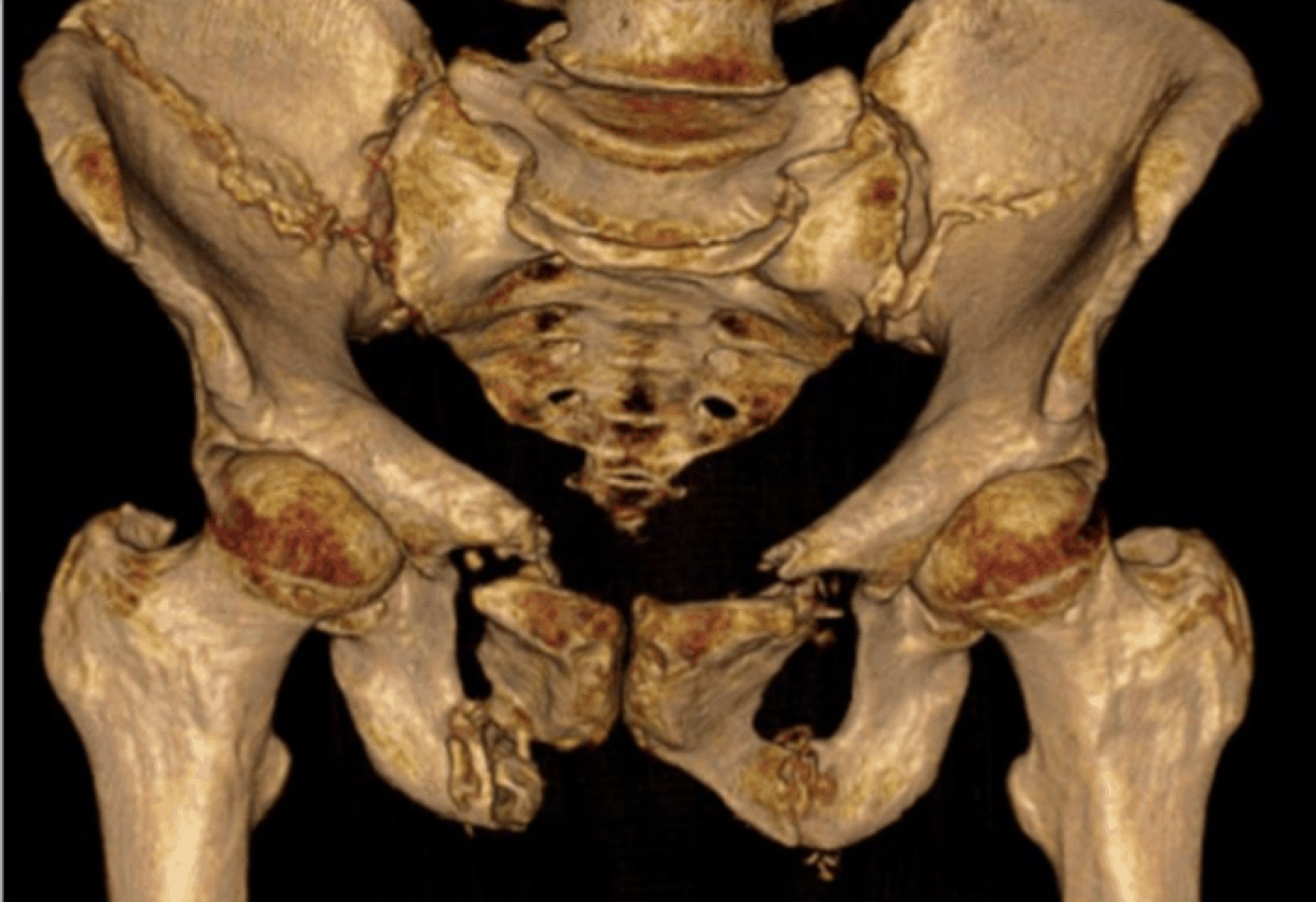
Pelvic fractures are most often associated with massive trauma. In terms of skeletal injuries they account for about 3% of all injuries. However they have the potential to result in haemodynamic instability, leading to significant mortality. Approximately 10 years ago the mortality from multi trauma with pelvic ring disruptions and haemorrhagic shock approached 60% (J Orthop Trauma 2002 16 : 553-61) Today that number is less than 20%
The instability from pelvic ring fractures results mostly from “open book” fractures. This is a direct result of the increase in pelvic volume that occurs with these, accommodating a larger volume of bleeding. Bleeding is usually venous from the pre sacral plexus (80% of cases) It may also be arterial from a branch of the internal iliac artery.
Searching the literature for the best approach to these unstable pelvic fractures, rapidly uncovers the fact that there are no randomised controlled trials. At best we have case series and case controlled studies. So at best level IV or V evidence. In fact there are less than 40 papers of relevance and most are retrospective studies. The approach to this patient group is mostly dealt with via consensus statements.
Mechanism of Injury
Pelvic fractures differ based on the direction of forces that cause the injury.
 Upward/ Downward Force – this causes a vertical displacement within the pelvis resulting in distraction at the pubic ramus and the sacroiliac joints.
Upward/ Downward Force – this causes a vertical displacement within the pelvis resulting in distraction at the pubic ramus and the sacroiliac joints.
 Anterior/ Posterior Force – this is the classical pattern of force in motor vehicle accidents. The result is, that it opens the ring.
Anterior/ Posterior Force – this is the classical pattern of force in motor vehicle accidents. The result is, that it opens the ring.
 Lateral Force– these forces cause the pelvis to collapse inwards. They close the pelvis and rarely cause haemodynamic instability.
Lateral Force– these forces cause the pelvis to collapse inwards. They close the pelvis and rarely cause haemodynamic instability.
Approach to the haemodynamically unstable pelvic structure
A set of simple questions allow a literature review in this area.
- What is the role of the pelvic binder?
- What role does FAST have?
- When is it time to go to theatre?
- What is the role of external fixation?
- What is the role of pelvic packing?
- What is the role of angiography?
What is the role of the pelvic binder?
 Pelvic binders reposition fractured parts, reducing pelvic volume and width, close to that achieved by definitive stabilization. (J Trauma 2005 Sept, 59(3) 659-64). It stabilises unstable fractures (Injury 2009 Oct 40(10): 1031-5) and can limit/ decrease venous blood loss. It should be applied and left in position, until there is fixation or haemorrhage control. The best position for the binder is over the greater trochanters and the pubic symphysis.
Pelvic binders reposition fractured parts, reducing pelvic volume and width, close to that achieved by definitive stabilization. (J Trauma 2005 Sept, 59(3) 659-64). It stabilises unstable fractures (Injury 2009 Oct 40(10): 1031-5) and can limit/ decrease venous blood loss. It should be applied and left in position, until there is fixation or haemorrhage control. The best position for the binder is over the greater trochanters and the pubic symphysis.
What role does FAST have?
The FAST abdominal ultrasound scan is used to ensure that there is no intraperitoneal compartment haemorrhage, that may be the cause of the haemodynamic instability. In some cases of retroperitoneal haemorrhage, there may also be blood in the peritoneal compartment
When is it time to go to theatre?
The hemodynamically unstable patient with a positive FAST study needs to go to the operating room. At this time they receive definitive treatment for intrabdominal injuries and the pelvis is stabilised. Whilst in the operating room the pelvis can also be packed.
What is the role of external fixation? What is the role of pelvic packing?
Pelvic packing on its own, is effective in controlling haemorrhage. ( Injury 2009 April 40 (4) 343-353) and its benefit extends to children and adolescents. ( J paediatric surg 2012 Dec, 47(12) 2240-50). The effectiveness if packing is increased when used with a C-clamp. (J Emerg Trauma Shock 2011 4 (4) 477-82)
Pelvic packing should be performed when a laparotomy is performed, or if there is a delay to, or lack of angiography services for embolization. When angio is delayed for more than 2 hours, pelvic packing decreases the need for blood transfusion over the next 24 hours and outcomes are improved ( Injury 2009 Jan 40(1) 54-60).
What is the role of angiography?
 Angiographic embolization controls arterial haemorrhage. It is lifesaving, as packing may control venous bleeds but doesn’t usually control arterial bleeds. It should be performed within 30-45 minutes. The procedure itself can be time consuming, which means that you will be working on an unstable patient in the angio suite. The procedure can be repeated if necessary.
Angiographic embolization controls arterial haemorrhage. It is lifesaving, as packing may control venous bleeds but doesn’t usually control arterial bleeds. It should be performed within 30-45 minutes. The procedure itself can be time consuming, which means that you will be working on an unstable patient in the angio suite. The procedure can be repeated if necessary.
Let’s put it all together
In a haemodynamically unstable patient with a Pelvic Fracture, a PELVIC BINDER is applied.
A FAST is performed.
If POSITIVE- the patient goes to theatre for laparotomy and pelvic stabilisation, as well as packing if required.
If NEGATIVE and Angio is available within 30-45 minutes, the patient goes to angio. If angio is not available, or will be delayed, the patient goes to theatre.
If the patient goes to angio and embolisation occurs and they are stable, they go to ICU.
If the patient has had pelvic packing and now stable, they will need a Contrast CT to look for a ‘blush'(arterial Bleed)
If you work in a centre where there is no angio and the patient is unstable, they should go to theatre for packing and a C-Clamp and then be transferred to a trauma centre with facilities.
Below is a Concensus Document from 2014 which reflects the management approach just described.