Syncope is one of those conditions you either love or hate. I certainly have at least five presentations of patients with syncope per shift. Having an approach to those patients certainly helps minimise missing the big stuff. Remember that syncope is a symptom and we need to find the diagnosis. The detective work is about getting the history right, looking for some select findings in the clinical examination and ordering some specific tests.
Definition of Syncope
In order to make the diagnosis we must have a definition. There are three parts to the definition of syncope:
- Sudden brief loss of consciousness
- Loss of postural tone
- Return to baseline
The patient will lose consciousness, in many cases following having a prodrome of some sort. The collapse is secondary to a loss of blood pressure. If they are standing, they will usually collapse, thus bringing the head to the same height as the heart and enabling perfusion. There will then be a spontaneous awakening, usually within about 30 seconds or so and a return to baseline i.e.., the person can go back to what they were doing prior to the incident.
Causes of Syncope
There are many causes, however I like to split them into causes that we can’t miss and those that we can send the patient home with.
REFLEX Syncope is considered a more benign form of syncope, although patients can still suffer injuries from falls.
This can either be
- Vasovagal syncope: An event secondary to a noxious stimulus, where the patient will become nauseated and diaphoretic and then lose consciousness or
- Situation syncope: It follows an event such as micturition or defecation, or carotid sinus massage.
CAN’T MISS DIAGNOSES
- Cardiac causes, which include anything that reduces blood flow i.e., ischaemia, cardiomyopathy, arrhythmias, valve issues
- PLUS diagnoses: These include
- Abdominal Aortic Aneurysm(AAA)
- Aortic Dissection
- Subarachnoid Haemorrhage(SAH)
- Pulmonary Embolism(PE)
I call these the PLUS diagnoses as the patient has SYNCOPE PLUS something i.e., syncope plus shortness of breath(PE), syncope plus abdominal or flank pain(AAA), syncope plus severe headache(SAH).
Could it have been a seizure?
In many cases the collateral history we get may include myoclonic jerking movement, which may look like a seizure. The key features in the history and the patient’s presentation are:
- Was the patient post-ictal? In most cases patients will regain consciousness within 30 seconds to one minute. The older the patient, the longer it takes. However if the patient has not returned to their baseline within approximately 5 minutes, this may be a seizure.
- Was there tongue bitting? Patient with a seizure will bite the lateral aspect of the tongue. Those with a syncopal episode may also bite their tongues, however it is usually the tip of the tongue that they bite.
- Has the patient been incontinent? This is usually a sign a seizure.
- Beware Todd’s Paresis. Patients may have neurological symptoms post a seizure that include a hemiplegia. Which leads to the question of whether a transient ischaemic attack(TIA) can cause syncope.
Could it be a TIA?
A TIA will not usually cause a loss of consciousness. In order for there to be a loss of consciousness, both hemispheres must be affected. In cases where there may be a posterior circulation TIA, which may cause a loss of consciousness, patients will have symptoms such as vertigo or ataxia.
BLEEDING can cause syncope
Some of the major causes of bleeding can also cause syncope. They include:
- Ectopic Pregnancy
- AAA
- Aortic Dissection
- Any Gastro-intestinal Bleed
Could it be a CARDIAC Cause?
Cardiac causes of syncope are very concerning, as cardiac syncope increases the risk of death from any cause. In fact the first thing I would ask is:“Was this episode of syncope due to a cardiac cause?” If not, I would then ask “Was this a syncope-plus cause ie., AAA, dissection, SAH or PE?”
Cardiac causes tend to be those that cause a sudden collapse with no prodrome. They are usually due to an arrhythmia, or outflow tract obstruction. We need to beware, because cardiac causes are not always sudden and they can sometimes be accompanied by a prodrome related to a slower lowering of blood pressure.
Who Are The HIGH RISK Patients?
When looking at the literature, there are three groups that consistently appear:
- Older age group(>45 yo)
- Those with a cardiac history, especially cardiac failure, or those with an arrhythmia history and
- Those patients with an abnormal ECG. This means anything other than normal sinus rhythm.
HISTORY, EXAMINATION AND INVESTIGATION
HISTORY
The history is paramount in patients with this presentation. We need to understand what was happening just before, during and after the event, as well as what the event looked like. For example, was this simple post micturition syncope that occurred within a minute or so of the patient going to the bathroom, or did the patient get chest pain, feel palpitations and then lose consciousness? Was there tongue-bitting or incontinence?
Has the patient commenced on a new antihypertensive for example, or is the patient pregnant?
Is this the first episode, or one of many and is there any history in the family of syncopal episodes or of sudden death. Here we try to find out about the Brugada, or Arrhythmogenic right ventricular dysplasia, or the Wolf parkinson White syndromes.
EXAMINATION
We need to be selective.
The vitals are immensely important. What is the heart rate and the blood pressure? Is the patient febrile? These may change the diagnosis significantly.
The cardiac exam should be selective. I would mostly be listening for murmurs such as mitral incompetence or aortic stenosis and signs of cardiac failure.
In the nearological exam; are there any deficits?
In the abdominal examination, beware of the pulsatile mass in the abdomen, or other abdominal pain. Perform a rectal examination looking for evidence of gastrointestinal bleeding.
INVESTIGATIONS
These are few.
- Perform an ECG and look for the ECG’s of syncope as shown below. A normal ECG indicates a lower likelihood of arrhythmia as a cause of syncope. It has a low yield i.e.,<5%, but when it is positive, you have the diagnosis.
- In a woman of childbearing age, a pregnancy test
- A haemoglobin and hematocrit, will give information on blood loss.
- Other tests may include a Troponin, if the patient had chest pain, or a CT brain if the patient had a sudden headache, or an aortogram if the patient had a sudden onset of ripping chest pain. Tailor the investigations to the history and the symptoms.
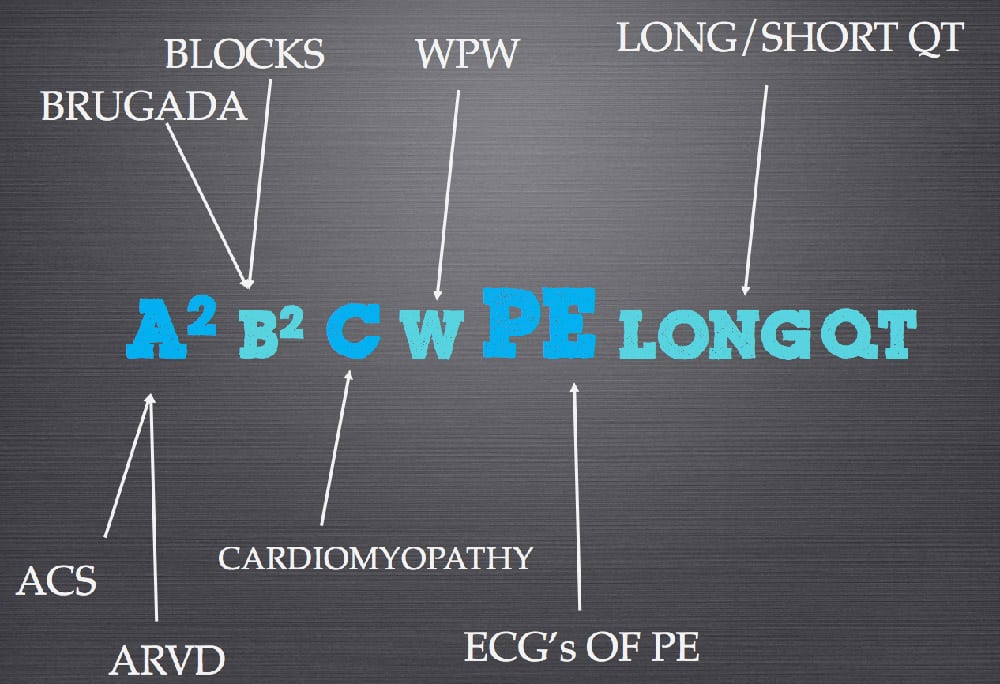
Below is the mnemonic I teach for the ECG’s of syncope.
![]()
The solution is shown below:
SYNCOPE SCORING SYSTEMS
There are syncope scores that we can use, to allow us to predict who will have potentially poor outcome.
San Francisco Syncope Score
This is perhaps the most famous of these. It is a validated score looking at 7 day adverse events, with a high sensitivity of about 98%, but a low specificity(56%). It can tell us that something bad will happen, it just doesn’t know what. The variables it uses include:
- Abnormal ECG
- Shortness of Breath
- Systolic Blood Pressure < 90mmHg
- Haematocrit < 30%
- Congestive Cardiac Failure
Oesil Risk Score
This looked at 1 year mortality and included risk factors that were each given a score. A total score of 4 risk factors had an associated 1 year mortality of 57.1%. The risk factors included were:
- Male
- Age >65yo
- Hypertension
- Cardiovascular disease history
- Diabetes
- Previous syncope
- Syncope without prodromes
- Syncope-related traumatic injurues
- Abnormal ECG
The Rose Score
This looked at one month outcomes and recommended admission if any of the following were present:
- BNP >300mcg/ml
- Bradycardia < 50
- Fecal Occult Blood
- Anaemia Hb < 90g/l
- Chest pain associated with syncope
- ECG with Q waves
- Saturations of < 94% on room air.
The were also others such as the Boston syncope rules.
The way to use the rules is as a check list before sending patients home. If I am about to discharge a patient I apply the San-Francisco syncope rule.








Another amazing job of Dr Peter Kass who guided me during my fellowship journey !
Thank you for the kind words Ali and your result was well deserved!