
Perimortem cesarian section is a rare and stressful procedure that must be performed in a timely fashion to give both the mother and foetus, the best chance for survival. Its rarity makes it something we must talk about, so that if any of us are faced with it, we know what to do. The fact that the procedure is a perimortem procedure affects us in so many other ways. It’s time that we stop thinking of this as a salvage procedure for the mother or foetus and start to think of it as a potential life saving procedure for both mother and foetus.
In 2015 Rose et al(Am J Obstetr Gynecol. 2015:213(5):653-6) coined the term ‘Resuscitative Hysterotomy‘, which reflects the benefit of the procedure to both.
In any pregnancy related trauma, all the other measures related to trauma need to be in place. There need to be a pelvic binder and blood products etc. If the foetus is greater than 20 weeks, the uterus must be displaced, either by tilting the patient or by manually displacing the uterus to the patient’s left.
The decision to perform this salvage procedure, must be made early so that preparations begin early. How early? Usually within a few minutes of commencement of resuscitation. The right time isn’t known; the literature is scant and the guidelines are consensus based. However we know that the chance of survival past the first five minutes drops significantly. It is sensible to perform the procedure prior to this time.
Things to Consider
-
The Gestational Age of the Fetus at Delivery
- There is controversy as to which foetal age we should be delivering.
- Assessing the foetal age in the resuscitation scenario, needs to be rapid. We know that when the fundus of the uterus is level with the umbilicus, that the age of the foetus is about 20 weeks. It then grows about 1cm per week above the umbilicus.
- If your uterus is above the umbilicus, that’s probably enough to proceed.
- It is accepted that a foetus of >23-24 weeks will will have the greatest chance of survival. It is also accepted that those less than 20 weeks will have poor survival. There is uncertainty in that group of 20-24 weeks.
- For all those where the foetus is less than 23-24 weeks Selden et al(Ann Emerg Med 1988 Apr 17(4)346-9) suggest that only aggressive maternal support is needed and the foetus should not be delivered, as it will be exerting only minimal haemodynamic effects on the maternal circulation.
- Rose et al(Am J Obstetr Gynecol. 2015:213(5):653-6) believe that regardless of the gestational age of the foetus, or time elapsed, if the resuscitation attempts are failing the foetus should be delivered.
-
The Time to Delivery
- This may be the most difficult thing to account for. Although some studies show successful deliveries occurring at 15 and 30 minutes following maternal cardiac arrest(Katz V et al Am J Obstet Gynecol 2005, June, 192(6): 1916-20), consensus opinion, is that delivery should occur within about 5 minutes.
- A 5 minute window for delivery effectively means that the decision has to be made at about 4 minutes. All preparations however should have begun on patient arrival. What if you go over that 5 minutes? It doesn’t really matter. Just get in there and do it. Case studies have shown success past the 5 minute mark.
The Procedure
- Perform a midline incision from the uterine fundus to the pubic symphysis
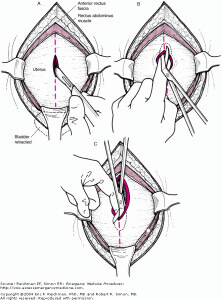
- Beware not to cut bowel, bladder or blood vessels
- Enter the uterine cavity, but only via a small cut
- Insert fingers into the uterine cavity and lift the uterus away from the fetus
- Use scissors to open the uterus, ensuring the foetus is not cut.
- Deliver the foetus:
- Easiest way is to find the head and get that out first.
- Suction nose and mouth
- Clamp the cord
- Resuscitation of both mother and foetus continues.
Post Hysterotomy
- Consider packing the uterus and the abdomen
- Consider putting manual pressure on the aorta
- Continue blood filling and resuscitative efforts
- Definitive closure, if the resuscitations successful, must be done in the operating room
- Have paediatrics close by with neonatal input, to resuscitate the neonate.
An Approach
- If the patient is expected, resuscitative hysterotomy must be discussed with the team.
- Get as much help as possible
- Get obstetrics down, if not then a surgeon at least
- Get paediatrics down, or if you have the expertise, a neonatal consultant
- Set up the equipment early, prior to patient arrival
- At minimum a scalpel, retractors, something for blunt dissection and surgical scissors. Apart from the retractors a normal suturing kit will have most of the equipment on it.
- Ensure uterus is displaced to the left during resuscitation
- Within 4 minutes of commencing resuscitation for cardiac arrest, if there is no reversal, then perform the procedure. Think of this as 2 cycles of CPR, or a non-shockable rhythm.
- If the uterus is above the level of the umbilicus, then perform the procedure.
- Post delivery, pack the uterus and abdomen as needed.
- Consider manually clamping aorta







I was recommended this web site by my cousin. I am no longer sure whether
this submit is written via him as no one else understand such certain approximately my problem.
You are amazing! Thank you!
Thanks on your marvelous posting! I genuinely enjoyed reading it,
you could be a great author.I will be sure to bookmark your blog and definitely
will come back down the road. I want to encourage
that you continue your great job, have a nice morning!
Hey there are using WordPress for your blog platform?
I’m new to the blog world but I’m trying to get started and set
up my own. Do you require any html coding expertise to make your own blog?
Any help would be really appreciated!
My homepage illegal drugs
Wow, awesome blog layout! How long have you been blogging for?
you made blogging look easy. The overall look of your web site is wonderful, let alone the content!
This web site is my intake, really great design and style
and Perfect written content.
my blog; stop smoking
Thanks to my father who shared with me concerning this website, this
web site is really amazing.
What’s Happening i’m new to this, I stumbled upon this I have discovered It absolutely useful and it has
helped me out loads. I am hoping to give a contribution &
aid other customers like its helped me. Good job.
Hi there, the whole thing is going nicely here and ofcourse every one is sharing facts, that’s genuinely good, keep up
writing.
Excelente post Dr Peter.
Didatico, objetivo e funcional.
Muito obrigado