Paediatric Resuscitation is stressful. However if we remember a few small points, it makes it so much easier. Here we specifically look at resuscitating children, not neonates.
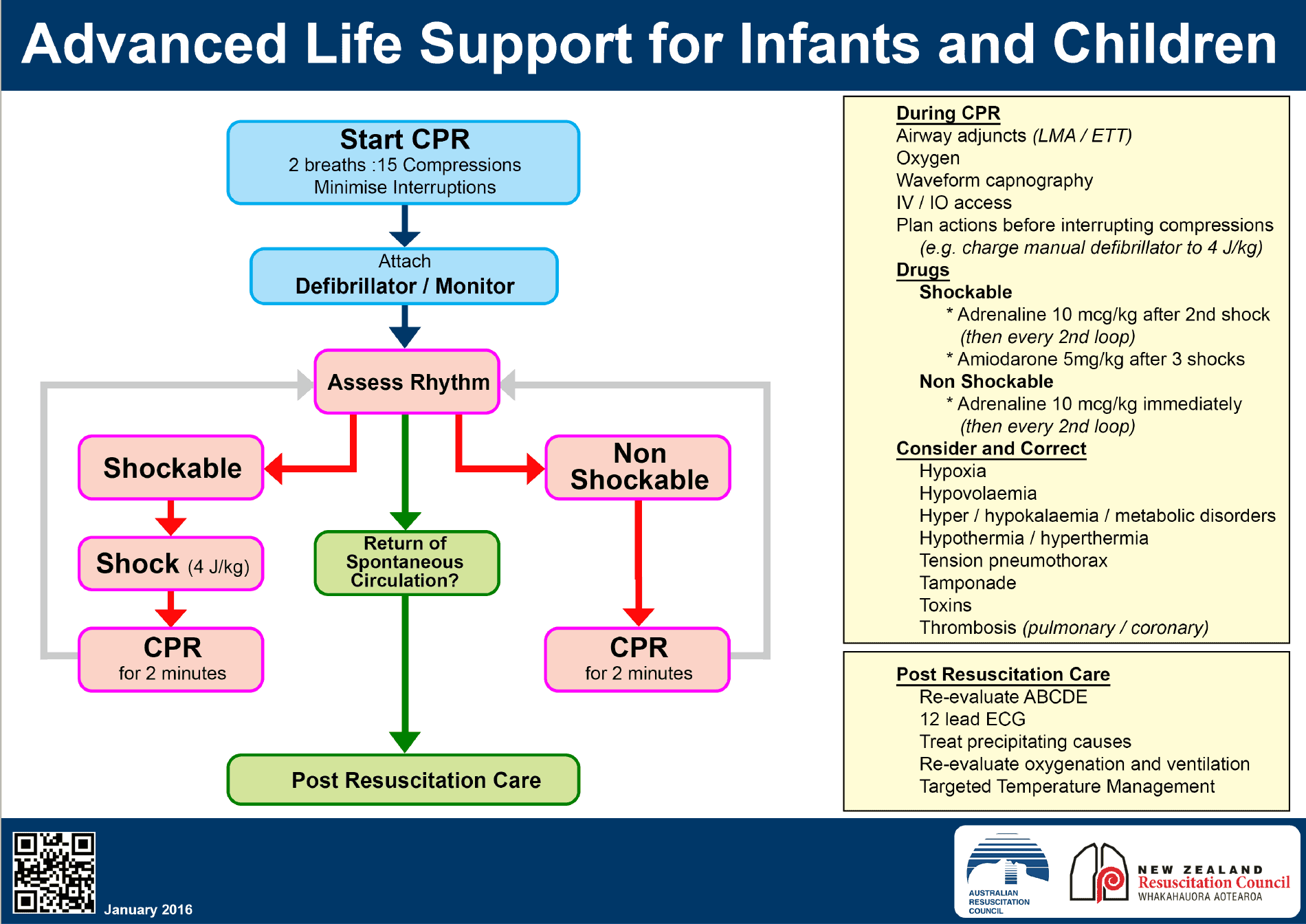
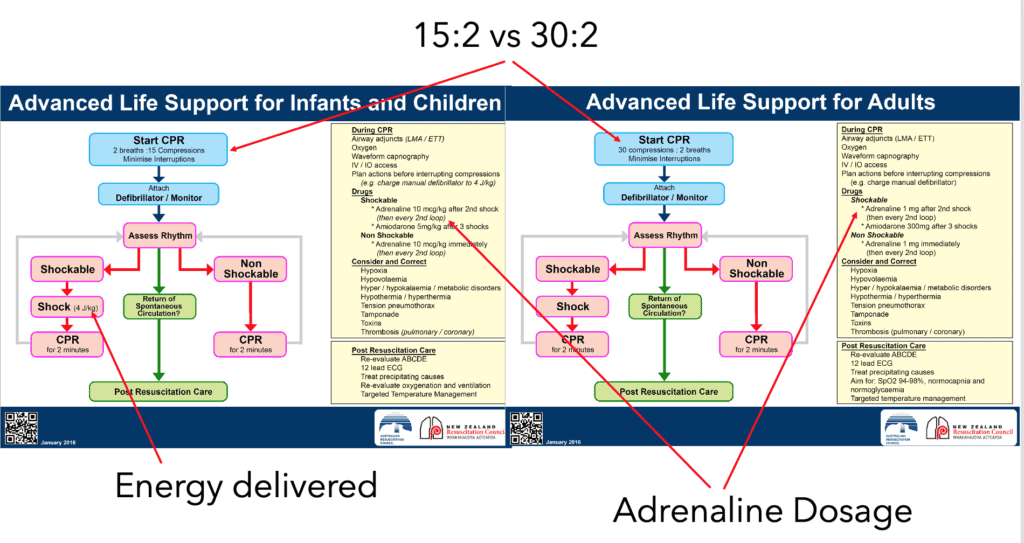
The Paediatric Resuscitation Guideline flowcharts have been purposefully made to look similar to the Adult guidelines, because the principles are the same. There are 3 main differences, discussed below.
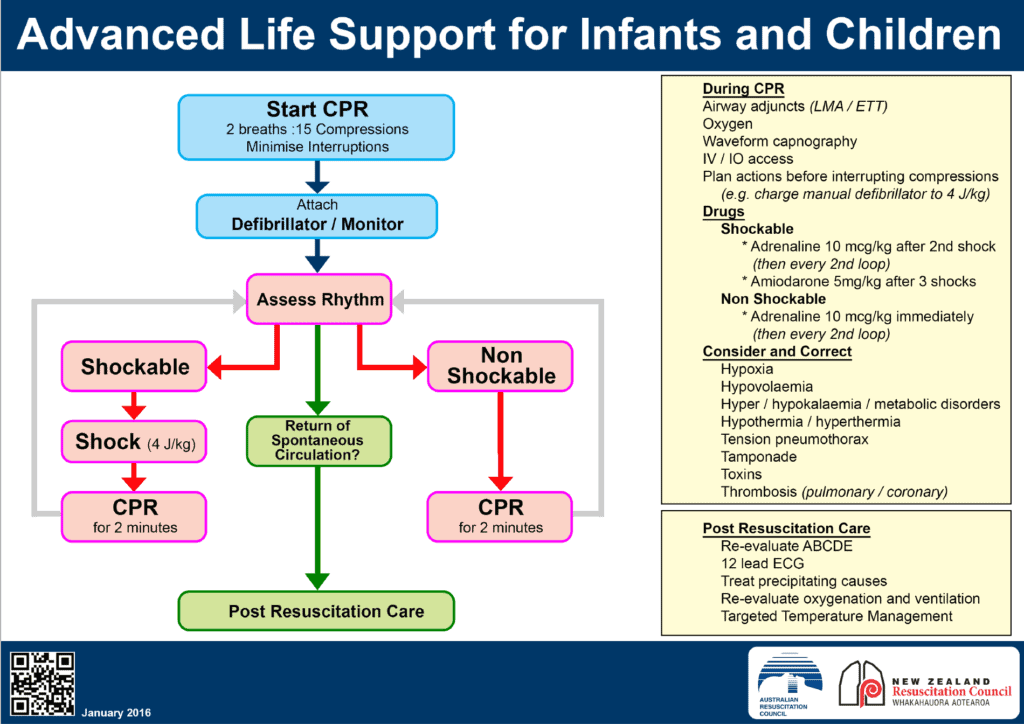
Differences Between Adult and Paediatric Resuscitation
Watch the video below, or read for the full notes
3 Differences between Adult and Paediatric Resuscitation
- Ratio of Chest Compression to Ventilation
- Adults 30:2
- Children 15:2
- Dose of Adrenaline
- Adults 1mg IV
- Children 10mcg/kg or 0.1ml/kg of 1:10,000 IV
- Energy dose in defibrillation
- Start at 2J/kg then go to 4J/kg, then again at 4J/kg, and even higher to 10J
There are 4 key points to make:
- For the purposes of resuscitation children are considered to be adults at age 8
-
In times of COVID we have had to change a lot of what we do. If we have a respiratory infection risk such as COVID, we need to assume everyone is COVID +ve, just as you would in adult patients. What occurs in times where there are other infection risks spread by respiratory droplets. The approach is the same:
-
PPE
-
Viral Filters
-
Airway by the most experienced person there
-
Closed Circuit(cuffed tubes)
-
- Most Pediatric Arrests are due to HYPOXIA and HYPOVOLAEMIA
- Treat for these and also think about about TOXINS
- Cardiac causes and PE etc., ie., the other H’s and T’s are not as common, unless the patient has a known condition
-
DON’T CALCULATE DOSES UNLESS YOU HAVE TO
-
Times of heightened stress lead to errors
-
Pre-calculate if you have to: If the patient’s age is know pre-calculate
- Make sure your calculations are checked
-
Use a Broselow Tape
-
Are Children just small Adults?
This has been up for discussion for some time now. There are those that unwaveringly say NO! However I believe that the gap is getting smaller in terms of our approach. Of course there are some differences, which comprise a small amount of paediatric specific knowledge we must have. It’s the adrenaline doses and the volume doses etc.
Most of us don’t work in dedicated paediatric emergency department, but see paediatric patients in mixed departments. For the paediatric specialists, it’s their ‘bread and butter’. For those that are occasionally exposed to a paediatric resuscitation, it can be very stressful.
The ability to think of children as small adults, I believe, makes it easier for us all to approach paediatric resuscitations; which I and I’m sure many of you, find stressful. It gives us the ability to clear our minds of the thoughts, that lead to the fear, that we know nothing about this patient group. It lets us move on with the resuscitation.
Back in 2016 I asked the Dr Bendall to speak on this topic. This is one of the best lectures I’ve heard on simplifying this stressful topic. It certainly gave me a new way of thinking.
Paediatric Arrhythmias
I think of cardiac arrest as being in one of three groups:
- TOO FAST: The tachycardics
- TOO SLOW: The bradycardics
- NOTHING AT ALL: Those that have no rhythm ie., asystole

TOO FAST
Children’s heart rates can be very fast. Early in life, children have lot of accessory pathways. It’s not uncommon to have rates above 200bpm.
The definition of tachycardia in children also varies with their age:
- < 2 year olds: >160bpm is considered fast
- 2-12 year olds: >140bpm is considered fast
- >12 year olds: > 100bpm is fast
Is It NARROW or WIDE?
Just as in adult patients, we need to ask the question “Is it a wide or narrow complex tachycardia?”
NARROW COMPLEX TACHYCARDIA
We can think of narrow complex tachycardias as falling into 2 main categories:
- Sinus Tachycardia
- Look for P waves to confirm
- Look for variability in rate. Remember that the ECG is a snapshot in time. Look at the monitor. If the rate varies it’s not an SVT
- In sinus tachycardia, treat the cause, which may be dehydration, or toxins or sepsis etc
- Supraventricular Tachycardia
- There are no P waves and the rhythm is exquisitely regular
- These patients need to be slowed down
- Vagal/Diving reflex
- Adenosine: Use 0.1 mg/kg followed by 0.2mg/kg
- If all else fails, and it usually doesn’t, DC cardioversion may be needed.
WIDE COMPLEX TACHYCARDIA
In adults there are multiple causes of wide complex tachycardia:
- Ventricular Tachycardia(80% of cases)
- SVT with Aberrant Conduction
- Bundle Branch Block
- Ischaemia
- Paced Rhythm
- Hyperkalaemia
- Na channel blockade
I think of the same causes in children. Obviously they won’t be paced etc, but it allows me to remember one list.
HOW WIDE IS WIDE?
In adults we consider >120ms (3 small squares) to be wide.
In children it is much narrower:
- >80ms in young children (2 small squares)
- >100ms in adolescents
IS THE PATIENT STABLE?
If the patient is unstable we need to progress to cardioversion and adrenaline as needed.
If the patient is stable, we have a short time to think. If there is a possibility of SVT with aberrant conduction and the rhythm is regular(ie not atrial fibrillation), we can try Adenosine. If it is an SVT, it will break. If not ie., if it is coming from the ventricles, the Adenosine should do nothing.
In the wide complex rhythms that we believe are VT we can progress to Amiodarone or cardioversion.

TOO SLOW
The second group I consider, are those children that come in and they are running too slow: Bradycardia.
Although there are multiple causes of bradycardia including heart blocks secondary to myocarditis, I assume that in most cases the cause is HYPOXIA. So I give oxygen.
Remember that if you are delivering oxygen by BVM, very young children may need assisted ventilation as they cannot generate forces high enough to open the ‘fish mouth’ valve when breathing.
If after about 1 minute of assisted ventilation and high oxygen delivery, the heart rate is below 60 bpm and the child is compromised, we commence CPR.
Adrenaline is the drug of choice to speed kids up (rather than Atropine).
Some children may need pacing.

NOTHING AT ALL (ASYSTOLE)
This is the most common arrest presentation.
We need to progress as we would with the adult patient:
- CPR
- Adrenaline
Think of the H’s and the T’s. However HYPOXIA and HYPOVOLAEMIA are the commonest causes. We’ve given oxygen. I also consider a bolus of fluid (0.9% saline) 10-20ml/kg
Conclusion
Simplify the way you think about cardiac arrest in children. It will reduce stress and make it easier to manage the resuscitation.







