
I don’t know about you, but I’ve always wanted to be able to perform a neurological exam and pick the lesion and look good doing it. Over the years I’ve tried to get better at it. What I have put together is a series of ‘PEARLS’ that sometimes help me decipher the cryptic world of Neurology. Here are a few.
1 ARM DRIFT
When holding the arms outwards, with palms upwards, three types of drift may occur:
- The Pyramidal Drift (Pronator Drift)
- The Cerebellar Drift
- The Parietal Drift
PRONATOR DRIFT (Barre’s Sign)
If you can perform only one test of upper limb motor function, this is the test to do. It can pick up subtle changes that would not be picked up by a routine motor examination.
 HOW TO PERFORM IT.
HOW TO PERFORM IT.
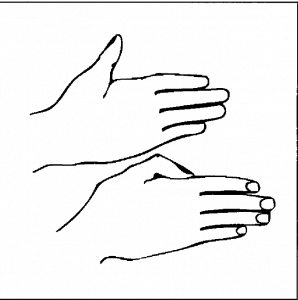
Ask the patient to extend both arms in front of them at shoulder height with palms facing upwards, as if they were carrying a tray. They first do this with eyes open for 10 seconds and then they hold the position and close their eyes and count to 10.
A Normal Response will result in either no movement, or a slight pronation of both sides ie., symmetrical.
This should be done with eyes open and closed as this test may be positive in both motor weakness and proprioceptive involvement.(1)
Eyes Open: If there is an upper motor neuron(UMN) lesion, the affected arm will pronate and drop. This occurs because in an UMN lesion that is not resulting in upper limb flaccid paralysis, may minimally affect the corticospinal tracts(CST). If these are affected, those muscles such as the flexors and pronators that are unaffected will overpower the weaker muscles ie., supination is weaker than pronation.
Eyes Closed: If the Pronator Drift is positive with eyes closed but not when the eyes are open there may be proprioceptive involvement ie., posterior columns.
CEREBELLAR DRIFT
In cerebellar disease the arm may drift up and outwards(usually towards the side of the lesion), or may drift aimlessly. A further test is overcorrection ie., give the palm or the arm a tap and it will overcorrect, never going back to its original position.
If there is a suspicion of cerebellar disease, move onto the rest of the cerebellar examination which will include:
- Speech
- Nystagmus
- Past Pointing(finger nose)
- Dysdiadochokinesia(rapid alternating movements)
- Rebound
- Heel-Shin
- Pendular reflexes
- Gait
Another form of the rebound test, other than tapping on the arm and seeing if it corrects appropriately, is to ask the patient to push or pull against you with their arm. You hold a constant amount of force against the limb, then suddenly let go(being careful not to injure the patient or yourself). Usually the antagonist muscles will stop the limb after a short movement. In cerebellar disease, the rebound phenomenon is absent and the arm will continue to move, hitting either you or the patient.
PARIETAL DRIFT
Upward and outward drift is specific for a contralateral parietal lesion. The parietal lobe is responsible for joint position sense and two point discrimination. When perfoming this test on someone with a parietal lesion, they cannot discern the position of their limb in space, with the result usually being an upward drift.(2)
CONVERSION DISORDER
 Downward drift of the arm without pronation, is usually the result of functional paresis. Conversion Disorder is a Psychiatric Disorder and the finding of ‘Pronation without Drift’ appears to be very sensitive and specific for this(3).
Downward drift of the arm without pronation, is usually the result of functional paresis. Conversion Disorder is a Psychiatric Disorder and the finding of ‘Pronation without Drift’ appears to be very sensitive and specific for this(3).
2 UPWARD THUMB SIGN
 In this test the patient is asked to hold their arms outstretched on their laps, with palms facing each other and thumbs resting on the index finger. They are then asked to raise them upwards quickly to shoulder level. Those with involvement of the corticospinal tracts have an upping thumb(4).
In this test the patient is asked to hold their arms outstretched on their laps, with palms facing each other and thumbs resting on the index finger. They are then asked to raise them upwards quickly to shoulder level. Those with involvement of the corticospinal tracts have an upping thumb(4).
It has been found to be a sensitive and reliable marker of UMN disease(5).
References
- Today I et al. Pronation Test: eyes closed or open? Eur Neurol. 2007;58(2):65-9.
- Raju S A et al. Distinguishing Motor Weakness from Impaired Spatial Awareness: A Helping Hand! Clin Med Insights Case Rep. 2017; 10
- Daum C et al. Validity of the “Drift without pronation” sign in conversion disorder. BMC Neurol. 2013; 13: 31.
- Hachinski V. The Upping Thumb Sign. Letters to the Editor.
- Hachinski V et al. Upping Thumb Sign. A sensitive indicator for brain involvement? Neurology. 2017 Jul 25;89(4):370-375








G’day Peter,
Thanks for your succinct and clear summary of Pronator Drift. Refreshing to see clinical engagement of examination and clinical reasoning before CT.
Thanks John
I especially like these when, the pronator drift does not fit the clinical picture ie., there’s no pronation. Then the full Neuro exam gets pulled out.
Neuro Exam Pearls: Upper limb – Resus
armzcrnhtbi
[url=http://www.g1k0nq5ugte7562728qqy047r79hj4jws.org/]urmzcrnhtbi[/url]
rmzcrnhtbi http://www.g1k0nq5ugte7562728qqy047r79hj4jws.org/
Appliance Toy
Paper Bag With Rope
Antique Decoration Wall Clock
Bath Tub Drain
Hermesエルメスマフラースーパーコピー
China Sf6
Hermesエルメス指輪スーパーコピー
LouisVuittonルイヴィトンサングラススーパーコピー
Good Stainless Steel Cookware
Art Kit
Diorディオールネックレススーパーコピー
Diorディオール靴スーパーコピー
squat type toilet
Hdpe Pipe Bends
LouisVuittonルイヴィトンマフラースーパーコピー
Lab Washer With Drying
Chanelシャネル帽子販売店
ブランドLouisVuittonルイヴィトンバッグコピーN級品
movable toilet
Bvlgariブルガリイヤリングスーパーコピー
4 Oz Spice Bottles
Glass Pipes And Bongs
IWCバッグコピー
Dc Line Noise Filter
ブランドDiorディオールマフラーコピー代引き
That poem made me cry. It’s so beautiful that you gave people a chance to feel like they can talk again. I’ve not read Speak yet but I intend to soon.I wrote a post here about my own personal experiences with books.
Buy Stainless Steel Sheet
ブランドコピー代引き
ブランド財布コピー
Mobile Concrete Mixing Plant
Pretty section of content. I just stumbled upon your web site and in accession capital to assert that I acquire actually enjoyed account your blog posts. Anyway I抣l be subscribing to your feeds and even I achievement you access consistently quickly.
Automatic Door Breakout System
ブランド時計コピー
ブランド時計コピー
Blow Molding Systems
Cystine Tablet
Balenciagaバレンシアガ靴コピー
Door Lock
ブランドTiffanyティファニーネックレスコピー代引き
ブランド財布コピー
Food Carts For Sale
Testosterone Steroids
Cartierカルティエスーパーコピー
Thc Oil Vaporizer Cartridge
ブランドベルトコピーN級品
Surgical Face Mask Making Machine
Tiffanyティファニー指輪販売店
Table Light
ブランドバッグコピーN級品
China Fire Hose Reel Pump
Hermesエルメスマフラースーパーコピー
10m Rgb Led Strip Lights
ブランドTiffanyティファニーブレスレットコピー代引き
Tiffanyティファニーイヤリングスーパーコピー
Dust Proof
ブランドGucciグッチサングラスコピー代引き
Manual Screen Press
Goyardゴヤール財布コピー
trousers
8 Strip Pcr Tubes
ブランド財布コピー
Silicone Fluid
コピー時計
ブランドバッグコピー
HPMC Construction Grade
Food Saver Zip Lock Bags
taper bearing 32006
ブランドコピー専門店
Adjustable Dumbbell Barbell