When and How to Perform a Lateral Canthotomy
A 35 yo woman presents to your rural emergency department. She has recently had eye surgery at a large tertiary centre and has been allowed home. Her presentation to the emergency department is:
- Increasing Headache
- Left Eye Pain
- There is proptosis of the eye
- Restricted Extra-Occular Eye Movements
- Decreased visual acuity
- Afferent Pupillary Defect
- Pressure in the affected eye of 40mmHg
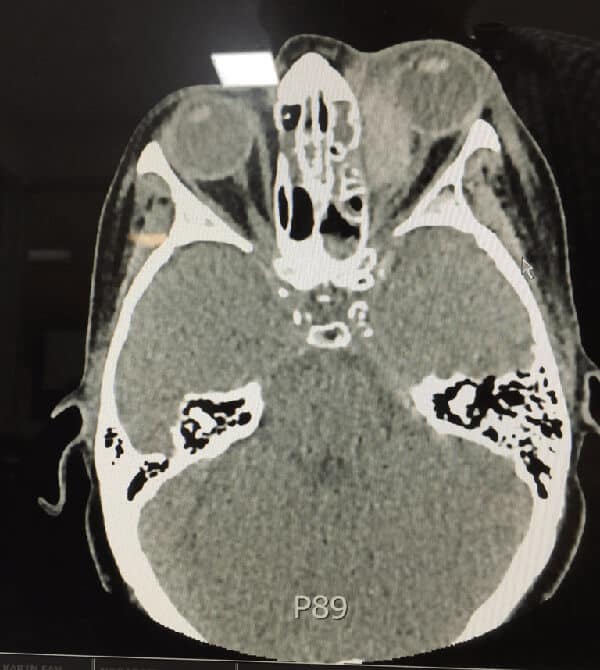
This is an ophthalmological emergency. In perfect world, the treatment should occur first, however because we did not know what was happening a rapid CT was done, which demonstrated a retrobulbar haematoma, causing the proptosis and a stretching of the optic nerve.
Usually if the pressures are <30mmHg, medical management is acceptable, however when the pressures reach 40 mmHg, there is a need for immediate decompression by lateral canthotomy and cantholysis.
The procedure should be performed by an ophthalmologist, however when no-one is available, it becomes an emergency medicine procedure.
Orbital Compartment Syndrome
The orbital compartment is a fixed space with limited capacity for expansion. If something like blood fills part of that space the pressure increases and may result in ischaemia of the optic nerve or the retina. A lateral canthotomy is a way of releasing this pressure.
You have up to approximately 2 hours before irreversible visual loss occurs. It may occur in less than 2 hours however, so speed is of the essence.
Indications for Lateral Canthotomy:
- Retrobulbar Bleed
- Decreased Visual Acuity
- Afferent Pupillary Defect
- Proptosis
- Increased Intra-occular Pressure- 40 mmHg and above of pressure requires decompression
Contraindications for Lateral Canthotomy:
A Potential Globe Rupture is the main contraindication. Findings that might point to that include:
- Hyphaema
- Irregular Shaped Pupil
- Subconjunctival Haemorrhage
- Enophthalmos
- Conjunctival Tear
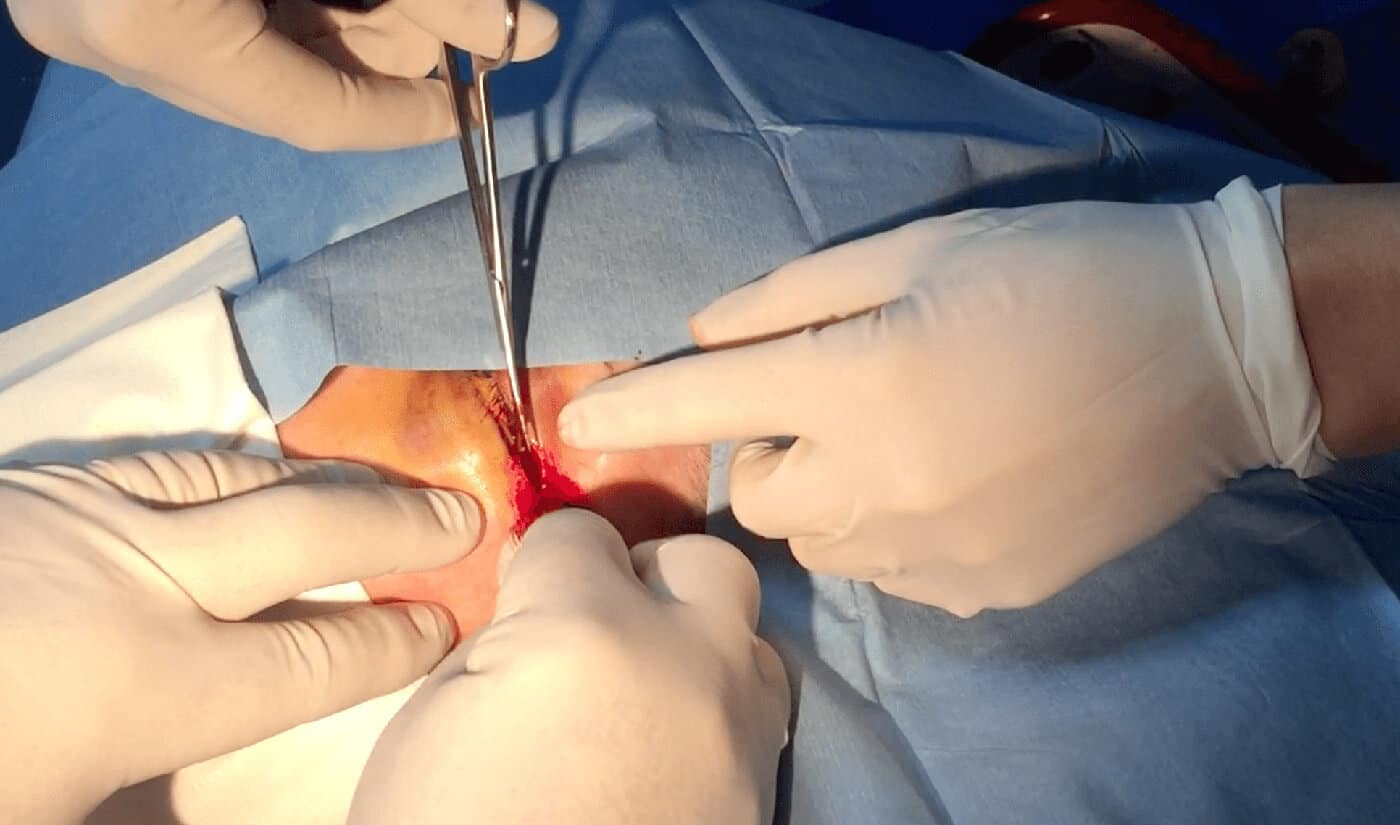
The Procedure
The procedure itself is relatively simple and is shown below in a video:
- Advise the patient and of what is to be done and get consent.
- Give gentle sedation. Our patient received 1mg IV midazolam, which was adequate
- Clean the area around the eye
- Inject 1-2ml of 1% lignocaine with adrenaline into the lateral canthus. Do not damage the globe

- Devascularise the Lateral Canthus: Use a small clamp to clamp the tissues for about 15-30 seconds.

- Make an Incision into the lateral canthus- staying away from the globe.

- Next cut the canthal tendons. These run superiorly and inferiorly and feel like guitar strings

There may be some bleeding, however this is easily controlled by direct pressure. The eye pressure should reduce almost immediately.
In our patient the eye pressure was measured within 5 minutes and had dropped to 29mmHg and then continued to drop further. The patient also had medical management including Diamox 250 qid and timolol eye drops.
Below is a video of the procedure:








It is easy procedure
Lateral Canthotomy – Resus
mfrzwrwkym http://www.gs1y4sl3v833q7ak754urs9b4j094t9cs.org/
amfrzwrwkym
[url=http://www.gs1y4sl3v833q7ak754urs9b4j094t9cs.org/]umfrzwrwkym[/url]
Hey! Someone in my Facebook group shared this site with
us so I came to take a look. I’m definitely loving the information. I’m
bookmarking and will be tweeting this to my followers!
Great blog and fantastic style and design.
Here is my webpage … A1 Keto BHB Ingredients
Really informative and wonderful complex body part of content, now
that’s user genial (:.
Feel free to surf to my blog post Extreme Keto
EFX Ingredients (http://www.hltkd.tw)
I got what you intend,saved to my bookmarks, very decent web site.
Feel free to surf to my web site … Nucentix Keto X3
I used to be able to find good information from your articles.
Feel free to visit my web blog :: TestoXmen Reviews (https://bbs.yunweishidai.com)
Hello to every body, it’s my first visit of this web
site; this website includes remarkable and genuinely good data designed for visitors.
Also visit my website :: Ultra Quick Keto Burn Review
I visit daily some web sites and sites to read articles,
except this website provides quality based content.
Here is my website – Extreme Muscle XXL Muscle Gainer (Clair)
Hey very cool blog!! Guy .. Beautiful .. Wonderful ..
I will bookmark your web site and take the feeds
also?I’m glad to seek out a lot of useful info right here within the publish, we need develop extra techniques on this
regard, thanks for sharing.
Feel free to surf to my web blog – Mega Male Enhancement Reviews
When someone writes an article he/she keeps the plan of a user
in his/her brain that how a user can understand it. So that’s why this paragraph is great.
Thanks!
Also visit my website – Tundra Breeze Portable AC Unit
Awesome website you have here but I was wondering if you knew of any discussion boards that cover the same topics
talked about here? I’d really love to be a part of community where I can get feed-back from other experienced individuals
that share the same interest. If you have any suggestions, please
let me know. Bless you!
Review my webpage … Erectesto XL Pills (polywebhost.com)
I think this web site has very fantastic composed content
material blog posts.
Also visit my blog post – Grown MD CBD
It’s really very complicated in this busy life to listen news on TV, so I just use web
for that reason, and obtain the newest news.
Visit my homepage :: Terra Xtract CBD Tincture
I’m really enjoying the theme/design of your website.
Do you ever run into any web browser compatibility problems?
A handful of my blog readers have complained about my site
not operating correctly in Explorer but looks great in Opera.
Do you have any advice to help fix this problem?
I saw a lot of website but I believe this one holds something special in it.
Also visit my web blog: Ultra Quick Keto Reviews
Very shortly this site will be famous among all blog
users, due to it’s pleasant posts
Feel free to surf to my page UltraXTend Wifi Extender
I loved as much as you will receive carried out right here.
The sketch is attractive, your authored subject matter stylish.
nonetheless, you command get got an shakiness over that you wish be delivering
the following. unwell unquestionably come more formerly again since exactly the same nearly a lot
often inside case you shield this increase.
you’re actually a excellent webmaster. The site loading pace is incredible.
It seems that you’re doing any unique trick.
Also, The contents are masterpiece. you’ve done
a magnificent activity on this subject!
コピー時計
China Stainless Steel Fitting
Seamless Mild Steel Tube
スーパーコピーブランド
Cigarette Lighter
スーパーコピーブランド
Diorディオールネックレス販売店
Dry Wipes
Concrete Pump Machine Diesel
ブランドFendiフェンディ靴コピー代引き
ブランドイヤリングコピー代引き
Rigid Core Vinyl Flooring
9×9 Fiberglass Self Adhesive Tape
Diorディオールバッグコピー
Ductile Iron Pipe Fittings Catalog Pdf
ブランド時計コピー
Bombshell Strapless Bra
ブランドPradaプラダ靴コピーN級品
ブランドコピー専門店
Guarantee Pvc Multicolor Mould For Kingsteel Machine
ブランドマフラースーパーコピー
Best Digital Dart Board
ブランドイヤリングコピー代引き
4 X 4 Cnc Plasma Table
Bvlgariブルガリブレスレット販売店
Melt Blown Fibers
ブランドChanelシャネルベルトコピー代引き
Flame Retardant Fabric
Chanelシャネルバッグ販売店
1000 degrees fire resistant sleeving
ブランド財布コピー
Lathe Parts
スーパーコピーブランド
China Dog Playpen and Dog Crate price
Led Solar Hanging Lights
コピー時計
Stainless Steel Hex Coupling Nut with Holes
Jasmine Bud Tea
ブランド財布コピー