Let me start by saying that some pulmonary embolisms(PE)’s are obvious. In those, you don’t need pulmonary embolism ECG findings to make the diagnosis. I recently was shown an ECG and asked what the patient’s diagnosis was. I asked my colleague, what the patient presented with. He replied;
“This is a 68 yo woman who presents with a sudden onset of shortness of breath. Her saturations on room air are 87%. She is afebrile and is in a new rapid atrial fibrillation. Her background history is metastatic cancer.”
My response,”She has a PE, why do I need to look at the ECG?” Correct, however it isn’t always this straightforward and in same cases, as shown in the literature, the ECG changes may be mistaken for ischaemia.
Let’s look at the ECG changes in PE
There are PE’s that are significant and those that aren’t. Most of us are walking around with PE’s and don’t know it. These are those sub segmental PE’s that the lungs clear. Perhaps then, the most common finding on ECGs is normal sinus rhythm.
Here is a list of finding on ECG in someone with a pulmonary embolism.
- Sinus tachycardia
- Supraventricular tachycardias such as SVT or PE
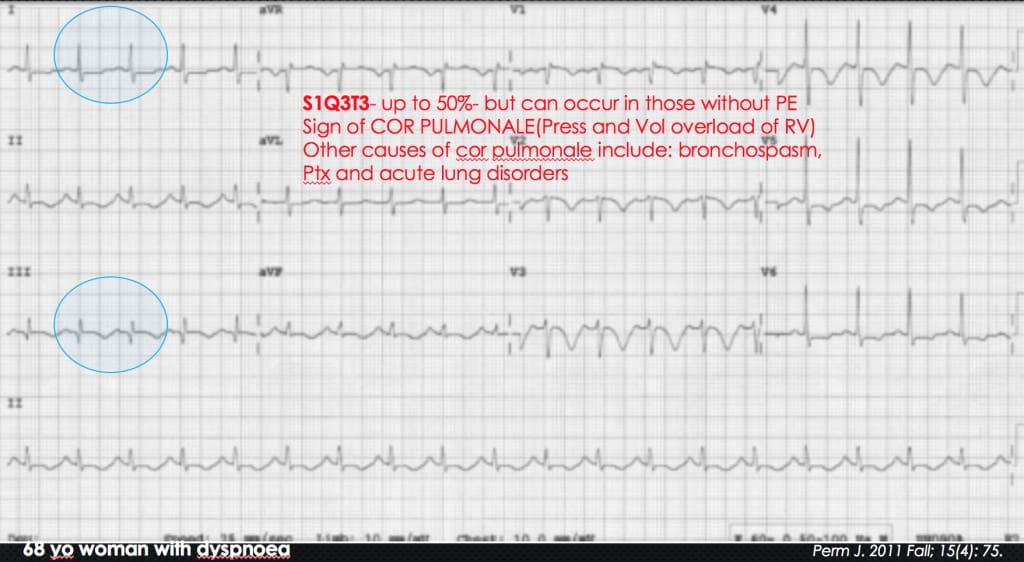
- S1Q3T3– up to 50%- but can occur in those without PE. It is a sign of COR PULMONALE(Press and Vol overload of RV). Other causes of cor pulmonale include: bronchospasm, Pneumothorax and acute lung disorders
- T wave Inversions in the anterior and inferior leads. The most specific finding.
- RBBB pattern
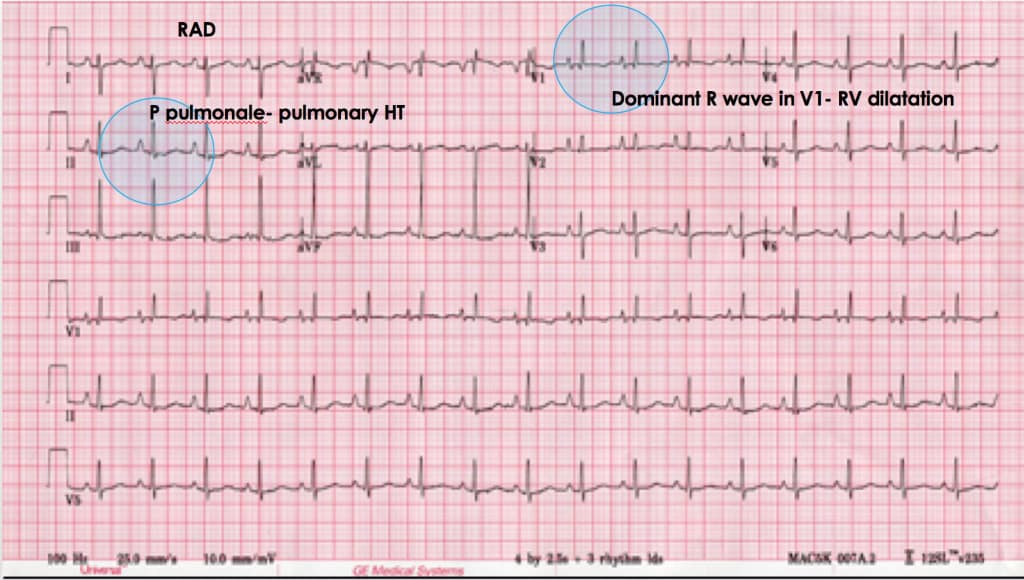
- Right axis deviation
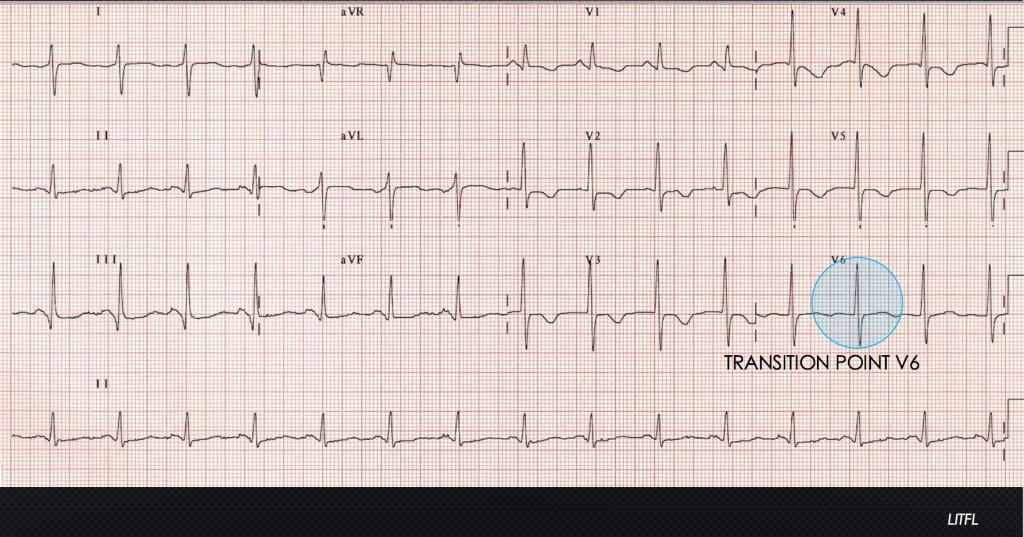
- Transition point shift
- P-pulmonale
- Dominant R wave in V1, indicating right ventricular dilatation
S1Q3T3
T wave inversion Inferiorly and anteriorly- most specific

Right Axis and Dominant R wave and P pulmonale
Transition Point shift
Watch the Video and come to Cardiac Bootcamp to learn about reading all critical ECGs.








The ECG’s of Pulmonary Embolism – Resus
[url=http://www.g2639ycvkd8q7744h2v8no50mu69z5kts.org/]ubdskpdslv[/url]
bdskpdslv http://www.g2639ycvkd8q7744h2v8no50mu69z5kts.org/
abdskpdslv
Amorphous Aluminum Silicate
Juki Sewing Machine Part
mobile restroom trailers for sale
best male masturbation device
Plastic Twine
Single Phase Common Mode Choke Power Filter
LouisVuittonルイヴィトン帽子スーパーコピー
Bow Hunting Gloves
LouisVuittonルイヴィトンサングラススーパーコピー
Low Noise Preamplifier
Anti Static Conveyor Belt
LouisVuittonルイヴィトンブレスレットスーパーコピー
LouisVuittonルイヴィトンネックレススーパーコピー
Cantilever Racking Suppliers
Class 900 Globe Valve
Fendiフェンディ靴スーパーコピー
Steel Coil Slitting Line
Celineセリーヌ財布スーパーコピー
Angler Kayak Paddle
Chanelシャネルサングラススーパーコピー
go outdoors portaloo
Chanelシャネル財布スーパーコピー
Loeweロエベベルトスーパーコピー
Drink Truck
Knitted T Shirt
Tiffanyティファニーブランドコピー代引き
ブランドRogerVivierロジェヴィヴィエ靴コピーN級品
Cemented Carbide Block
Personal Elevator
スーパーコピーバッグ
ブランド時計コピー
316l Seamless Tube
ブランドBalenciagaバレンシアガ帽子コピーN級品
Door Handle Child Lock
LouisVuittonルイヴィトン帽子コピー
Air Cargo Inspection Facility
Hdpe Blind Flange
Diorディオールサングラス販売店
High Pressure Automatic Green Sand Casting Supplier
ブランドGoyardゴヤールバッグコピーN級品
China Besuper Eco Diaper Garbage Bad
Bvlgariブルガリネックレス販売店
Teflon Cloth
LouisVuittonルイヴィトンネックレス販売店
Fendiフェンディ帽子販売店
aluminium checker plate suppliers
Burberryバーバリー靴コピー
Art Candles
ブランドコピー代引き
dettol kn95
Goyardゴヤールバッグスーパーコピー
Ceramic Bn Nozzles
ブランド時計コピー
Neptune Pipette Tips
ブランド時計コピー
Methyl Dichlorosilane
ブランドコピー代引き
220v Arc Welder
laser,hot cutting machine
ブランド財布コピー
Cnc Prototype Parts
ブランド財布コピー
Bathroom Double Sink Units
ブランドコピー専門店
Dosage of HPMC
Reflective Paracord
ブランドコピー代引き
5mm To 6mm Shaft Coupler
Pcr Instrument
ブランドコピー代引き
28610RKE004
Aluminum Corrugated Composite Panel Manufacturers
ブランドバッグコピー
Flat Pack Cabinet