A 19 yo male, University student presents with stabbing chest pain, with a pleuritic component. The pain radiates down his left arm. The pain started last evening but subsided, but has recurred again this morning, so he presents at 10 hours post pain onset to the emergency department.
The ECG is shown below. Please describe and interpret it.
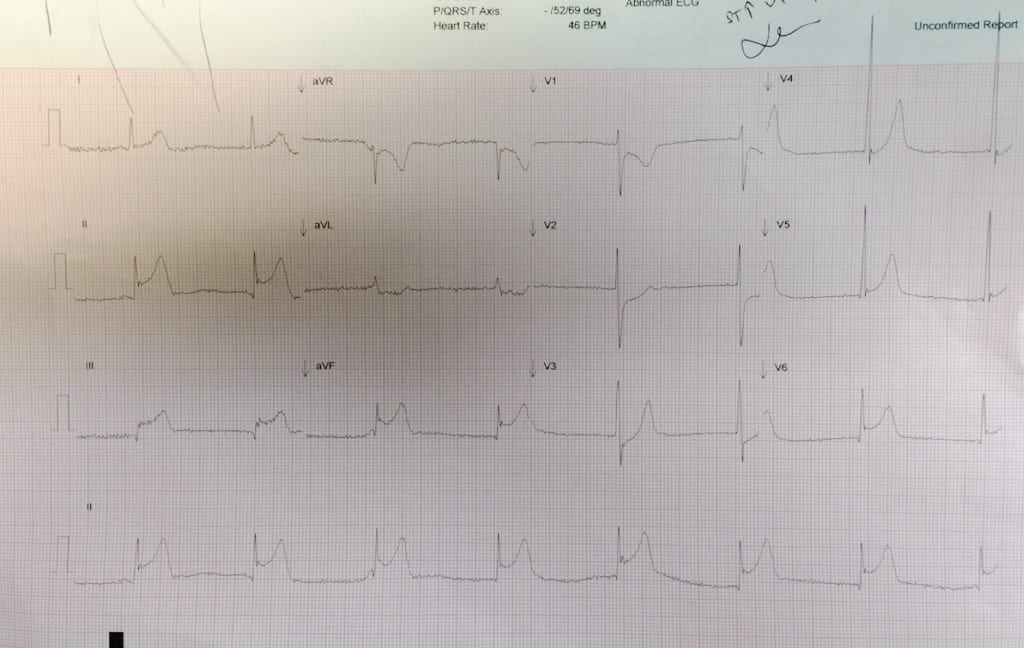
Describe the ECG
RATE: 8 x 6= 48
P WAVES:Upright in II and inverted in aVR. No extra p’s
QRS’s: Tall criteria for hypertrophy met S in V2 + R in V5 >35mm
ST-T: There is ST elevation in II, III, aVF, V5- V6, ST depression in aVL, V1-V3
INTERVALS:All normal
PACING: Nil pacing spikes seen
There is widespread ST elevation, however there are also reciprocal changes. When there are reciprocal changes, ischaemia must be considered. However most people would have to say that pain that has gone on for so long in such a young person must be pericarditis. There was no pericardial effusion on emergency echo.
The ECG was shown to a cardiologist who asked for thrombolysis, which was given. Post thrombolysis, the ECG was the same, however the pain resolved.
The Initial Troponin I is 9.1 and later that evening increases to > 50
Conclusion
MYOPERICARDITIS
It can present with fevers, myalgias and acute respiratory illness. It may be preceeded by respiratory illness or gastroenteritis. Chest pain may be similar to ischaemic pain.
The ECG can show widespread ST segment elevation and PR depression. There may also be:
- Inferolateral or anterolateral ST elevation and T wave inversion.
- Arrhythmias: SVT, non-sustained VT, ventricular ectopics.







