
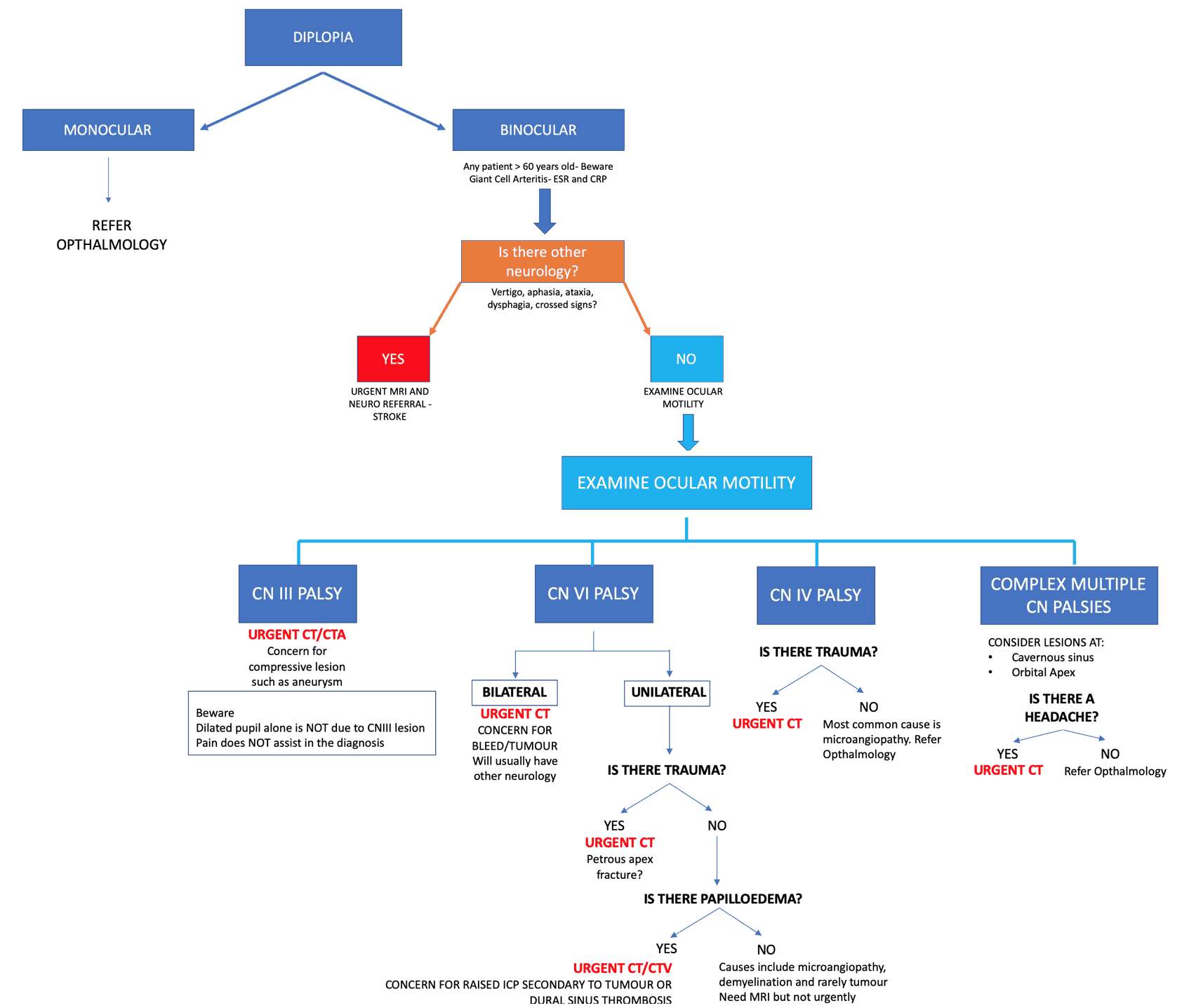
A patient presenting to the Emergency Department with diplopia can be a diagnostic challenge. Which patients need urgent imaging and which patients can be referred to outpatients? What is the imaging of choice? A recommended approach is shown below(1):
As a summary: If it’s Binocular PLUS any of the abnormalities below, perform a CT brain PLUS CTA or CTV as needed(explained below):
- Other neurological abnormalities
- Head trauma
- CN III abnormality
- Bilateral CN VI abnormality
- Papilloedema
- Headache
An Approach
The complete approach is shown below(Image 1) and can be downloaded as a PDF at the end of the blog. Here we break it up into parts for analysis.
Let’s break this down to simplify it
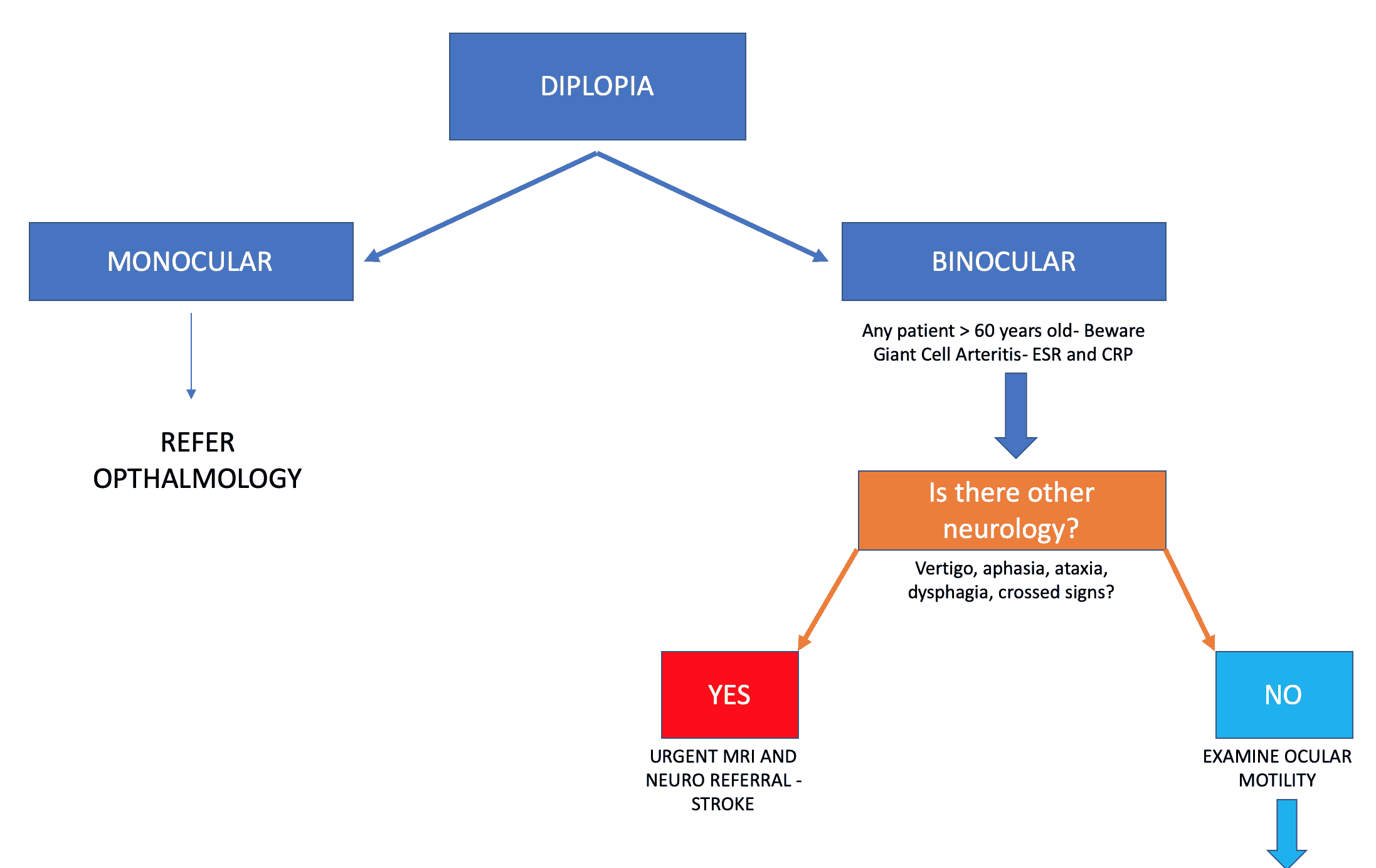
Is it Monocular or Binocular?

Monocular Diplopia
This does NOT resolve when one eye is closed or covered. The very fact that it does not resolve when one eye is closed indicates that it is NOT due to ocular misalignment ie ocular muscle issues.
The cause is almost all cases due to a refractive error or dry eyes. Patients should be referred to ophthalmology.
Binocular Diplopia
Binocular diplopia resolves when one eye is closed or covered. This indicates that ocular misalignment is the cause. Pathology may be related to:
- Ocular motor nerve pathology of cranial nerves(CN) III, IV or VI, either in the orbit or extracranially
- Restriction of movement of extra ocular muscles due to some other process
- Thyroid orbitopathy
- Orbital tumour
- Neuromuscular junction pathology eg myasthenia gravis
If Binocular, are there other neurological symptoms?
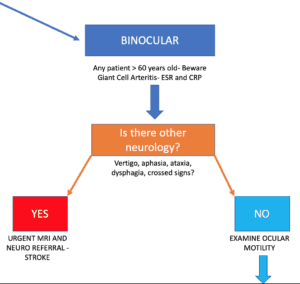
We need to especially look for brainstem symptoms(Image 3) such as:
- vertigo
- aphasia
- ataxia
- dysphagia
- crossed signs ie ipsilateral eye and contralateral hemiparesis.
In summary:
If it is ISOLATED Diplopia, we need to examine ocular motility
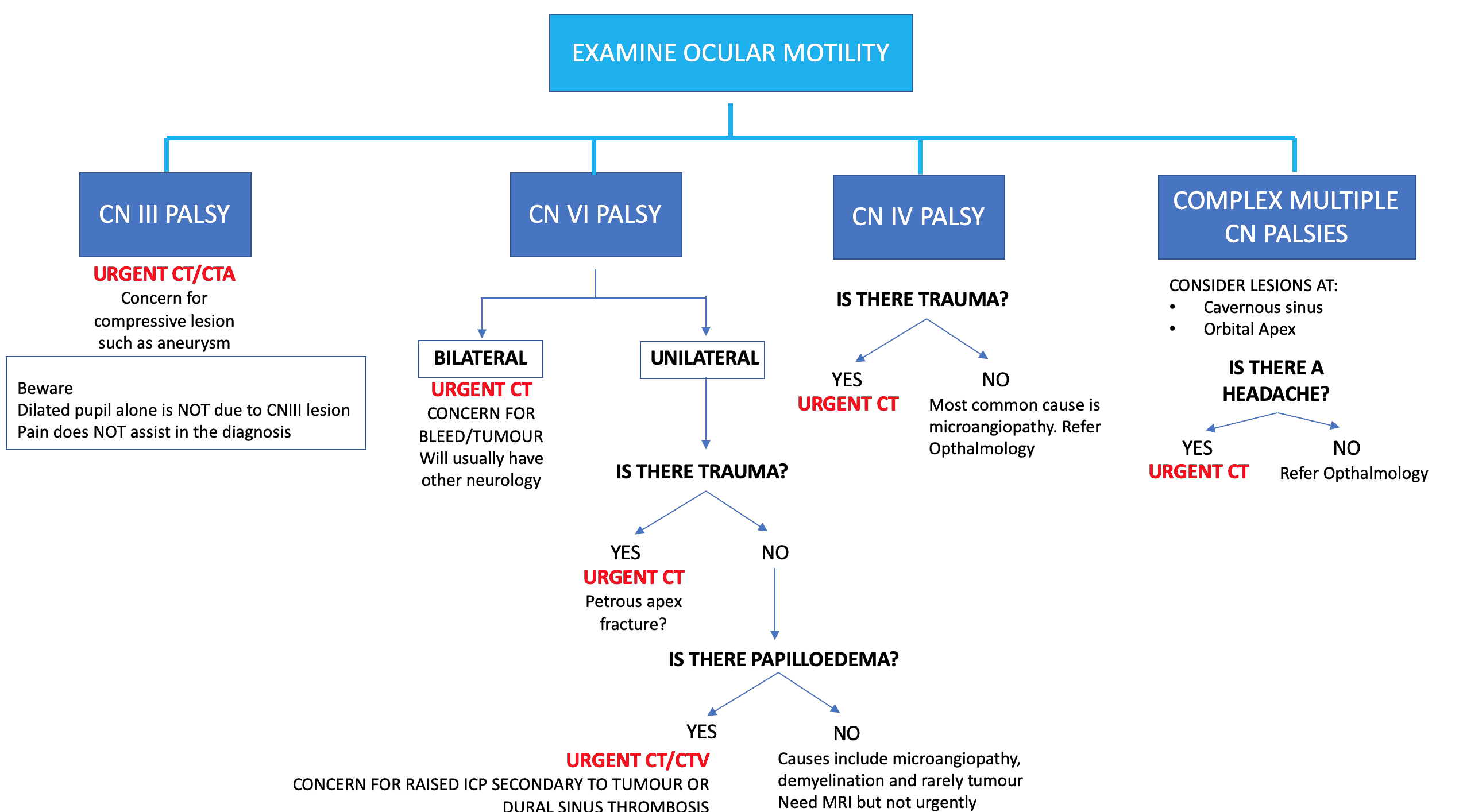
Let’s look at this in detail:
CN III
- The superior branch of the nerve innervates the ipsilateral superior rectus and lavator muscle.
- The inferior branch innervates the ipsilateral inferior and medial recti, the inferior oblique and the sphincter of the iris.
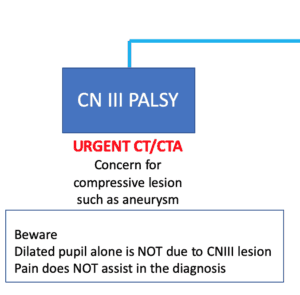
A complete CN III palsy will result in mydriasis, ptosis and a ‘down and out’ eye ie., cannot look up or medially. Palsies can be incomplete. However isolated anisocoria(dilated pupil) with no other extra ocular muscle involvement is bot due to CN III(2).
Patients with a CN III palsy require and urgent CT and CTA(Image 6), as up to 6% of cases are due to a compressive aneurysm(3).
CN VI
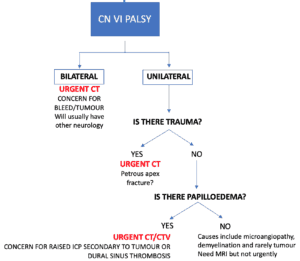
CN VI innervates the ipsilateral lateral rectus muscle.Patients present with esotropia(interning of the eye). Diplopia is worst when looking to the affected side and looking into the distance.
It is usually unilateral, as bilateral causes such as intracranial bleeds or tumours will usually present with other neurology. In patient with bilateral CN VI palsies an urgent CY brain is required.
Unilateral CN VI palsies are usually associated with(Image 7):
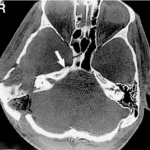 Trauma: Inpatients with trauma an urgent head CT should be done, looking for a petrous apex fracture(4). As CN VI leaves the brainstem it crosses the upper edge at the tip of the petrous bone, as seen in the image 8(5).
Trauma: Inpatients with trauma an urgent head CT should be done, looking for a petrous apex fracture(4). As CN VI leaves the brainstem it crosses the upper edge at the tip of the petrous bone, as seen in the image 8(5).- Microangiopathy, demyelination and neoplasm(rare): these patients require an MRI, although this may not need to be done as an emergent procedure.
Beware the patient with papilloedema. These patients need an urgent CT and CT venogram looking for an intracranial mass or dural venous thrombosis.
CN IV
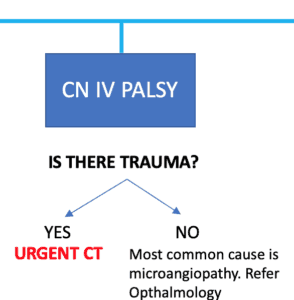
CN IV palsies can be difficult to diagnose as they are sometime vey subtle. Patients will have a vertical or oblique diplopia(Image 9). The most common causes are:
- Trauma: A CT brain should be performed as this nerve has the longest intracranial course.
- Microangiopathy: An outpatient review by ophthalmology is needed.
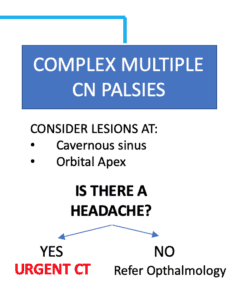
COMPLEX, MULTIPLE CN PALSIES
If more than one cranial nerve appears to be involved, then potential causes include(Image 10):
- Microangiopathy
- Cavernous sinus Lesion: It is important to consider pituitary apoplexy in any patient with headache. Eye findings are usually bilateral, due to communication and the patients are usually unwell(6). Read the case of bilateral hemianopia in pregnancy.
- Orbital apex lesion: Beware the patient with ophthalmoplegia plus decreased vision plus sensory deficit in V1 and V2 CT imaging is required to exclude a mass(7).
Putting it all together:
Download the PDF Approach to Diplopia
References
- Margolin E et al. Approach to a patient with diplopia in the Emergency Department. J Emerg Med. 2018 Jun;54(6):799-806. Pubmed
- Gross JR, et al. An approach to anisocoria. Curr Opin Ophthalmol 2016;27:486–92.
- Fang C et al. Incidence and etiologies of acquired third nerve palsy using a population-based method. JAMA Ophthalmol 2017;135:23–8.
- Koskas P et al. Towards understanding ocular motility: III, IV and VI. Diagn Interv Imaging 2013;94:1017–31.
- Mehmet FO et al. Isolated abducens nerve paresis associated with incomplete Horner’s syndrome caused by petrous apex fracture–case report and anatomical study. Neurologia medico-chirurgica 2001 DOI:10.2176/nmc.41.494
- Khatri IA, et al. Septic cerebral venous sinus thrombosis. J Neurol Sci 2016;362:221–7.
- Robinson D, et al. Orbit and orbital apex. Otolar- yngol Clin North Am 2011;44:903–22. viii.








Diplopia – Resus
spmhiigoxo http://www.g9n1s81vsc23407s108r65yeuphln5l1s.org/
[url=http://www.g9n1s81vsc23407s108r65yeuphln5l1s.org/]uspmhiigoxo[/url]
aspmhiigoxo
Automatic Floor Cleaning Robot
Burberryバーバリーバッグコピー
ブランドコピー代引き
Led Bathroom Downlights Ip65
Chanelシャネル財布コピー
Bulk Stone Manufacturer
China Disposable Face Mask
ブランドCartierカルティエイヤリングコピー代引き
Clear Zinc Oxide Powder
(TRIMETHYLSILYL)ETHYLENE
ブランドバッグコピー
Plastic Industrial Parts Injection Molds
Two-stage Telescopic Hydraulic Cylinder
ブランド時計コピー