
This is a great case that highlights how important it is, to know how to check if your ECG lead placement is correct. It also includes a rare case of dextrocardia.
CASE
A 39 yo male presented to the Emergency Department with crushing chest pain, that was associated with diaphoresis and shortness of breath. There was no cardiac history.
He was afebrile and his other vitals were: BP 138/107, heart rate 55bpm, RR 18 breaths per minute, SpO2 94% on room air.
Hi ECG is shown below(1):
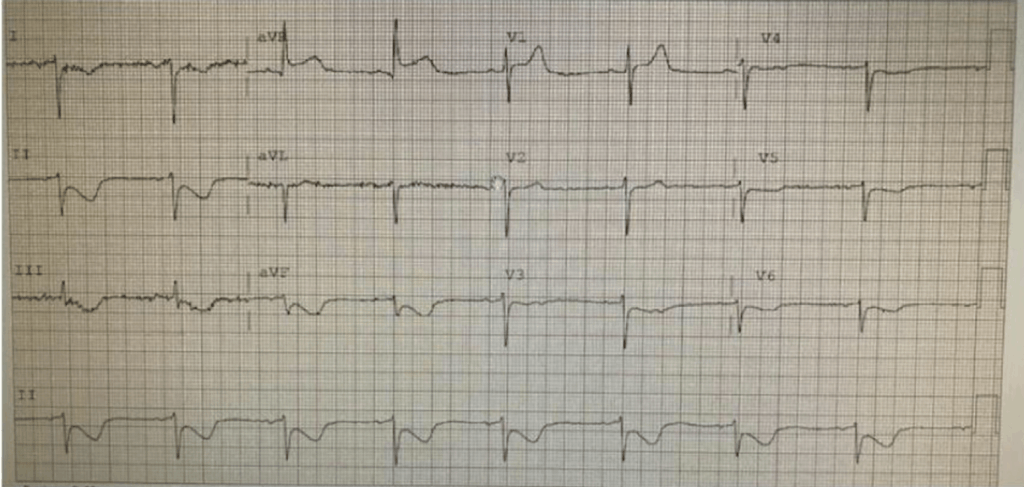
The ECG shows inferior lead ST depression with ST elevation in aVR. It was identified as ischaemia.
One of the first things to look for in an ECG is to see if it is in sinus rhythm ia the wave axis. The p waves must be upright in I and II and inverted in aVR. If they are not, the most common cause is limb lead reversal. The other cause, very much rarer, is dextrocardia. The other thing to note here, is the poor R wave progression.
The p waves here are upright in aVR and inverted in I and II.
Cardiac examination was performed and demonstrated a cardiac impulse on the right side of the chest.
Leads were then reversed and another ECG was taken as shown below:

With the precordial leads placed on the right side of the heart, the ECG now shows an ST elevation lateral infarction with reciprocal ST changes inferiorly. It was an important pick as we have gone from ST depression to an ST elevation MI.
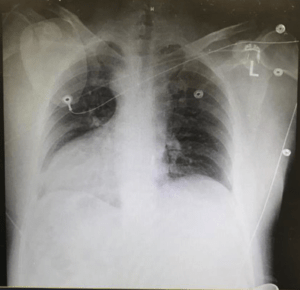
The dextrocardia was confirmed by chest xray. The patient went on to have cardiac catheterisation which demonstrated a 99% left main coronary artery stenosis and 70% stenosis to the obtuse marginal artery.
Reading the p waves in the limb leads to determine that they are placed correctly can change a diagnosis significantly. Here is a case I had a little while ago. A 25 yo male who presented with atypical chest pain. His ECG is shown below:
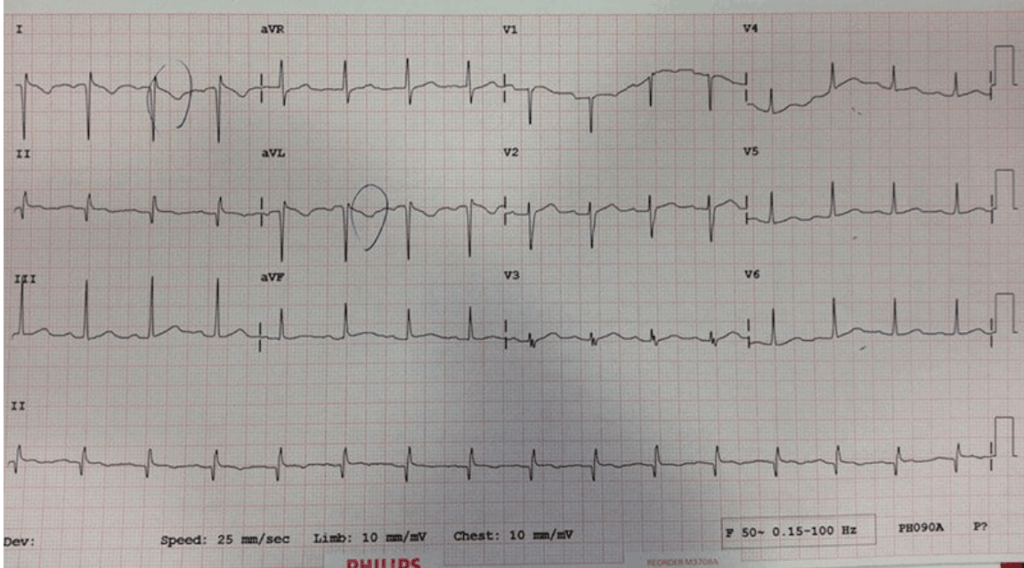
This case is concerning as there are T wave inversions in I and aVL. However the pain was atypical.
What do you think of the ECG?
When looking at the p waves in I, II and aVR, they are upright in aVR and inverted in I, the opposite of what is expected in sinus rhythm. Go to the case and see what happened when the leads placement was corrected.
Reference:
Elliot S et al. ST-Elevation Myocardial Infarction in a Patient Having Dextrocardia with Situs Inversus. The Journal of Emergency Medicine, Vol. 58, No. 5, pp. 797–801, 2020







