
Can Bedside Ultrasound be a Tool in the Assessment and Management of Renal Colic?
Bedside ultrasonography (BUS) has become a significant tool in the diagnostic repertoire of the emergency physician in recent years. Over the same period the use of, and potential risks of, CT imaging have come to the fore. Since the mid-1990s CT has been the mainstay of imaging for nephrolithiasis as it has high sensitivity and specificity (97% and 96% respectively {1}). Many patients with nephrolithiasis have repeat presentations and many undergo multiple CTs which lead to a significant cumulative radiation dosage.
In Emerg Med J 2013;30:3-8 Dalziel and Noble looked at a review of the literature on bedside ultrasound and suggested an algorithm for the management of renal colic patients in the emergency department. The paper contains some interesting data relating to the likelihood of a stone spontaneously passing based upon its size, see table 1.
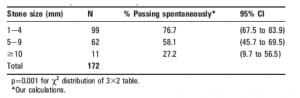
Table 1:Proportion of stones spontaneously passing dependent of size of stone identified by CT. (2)
They also quoted five studies that measured the accuracy of BUS for detecting hydronephrosis or stone disease. In these studies the sensitivity for detecting hydronephrosis ranges from 72% to 97% and specificities from 73% to 83% compared with either CT or IVPU as a gold standard (3,4,5,6,7).
Interestingly, the study by Henderson and colleagues had a higher sensitivity than the others for detecting hydronephrosis (3). Part of their protocol was the administration of 500 ml of intravenous fluid prior to scanning. Often the patient with renal colic can be mildly dehydrated due to vomiting or decreased oral intake. This may transiently collapse the pelvic collecting system and the administration of a fluid bolus may therefore unmask a previously obscured hydronephrosis, which could account for improved sensitivity in these patients.
The authors looked papers that correlated the degree of hydronephrosis visible on bedside USS with the size of stone and rate of clinically significant complication. They concluded that there was a significant correlation between degree of hydronephrosis and clinically significant stones.
To quote the authors “To phrase it in clinically meaningful terms, in Goertz’s (8) study the odds of having a stone <5 mm with mild hydronephrosis is 6.8:1 compared with 1.8:1 with moderate/severe hydronephrosis. The implication of this is that, in patients with stone disease and only mild hydronephrosis at BUS, we may need eight CT scans to identify one patient with a stone ≥5 mm in whom we might change our management. In those with moderate to severe hydronephrosis this number is closer to three. This suggests that mild hydronephrosis may indicate patients for conservative ED management when stones are considered the likely diagnosis, without the need for further imaging.”

A suggested algorithm for the management of renal colic patients in the emergency department (adapted from Swadron and Mandavia{9}). IVP, intravenous pyelography; KUB, kidney–ureter–bladder x-ray; US, ultrasound.
This algorithm appears to be well supported by the evidence and will assist in the management of nephrolithiasis in the emergency department whilst limiting radiation exposure.
by
Will Davies







