The ABG is one of the most basic tests we run in the Emergency Department.
It may be an ABG or a VBG. Regardless, it is an opportunity to gain information quickly.
This module will assist you in learning to read the ABG.
Look for my overall approach to the ABG at the end of the exercise
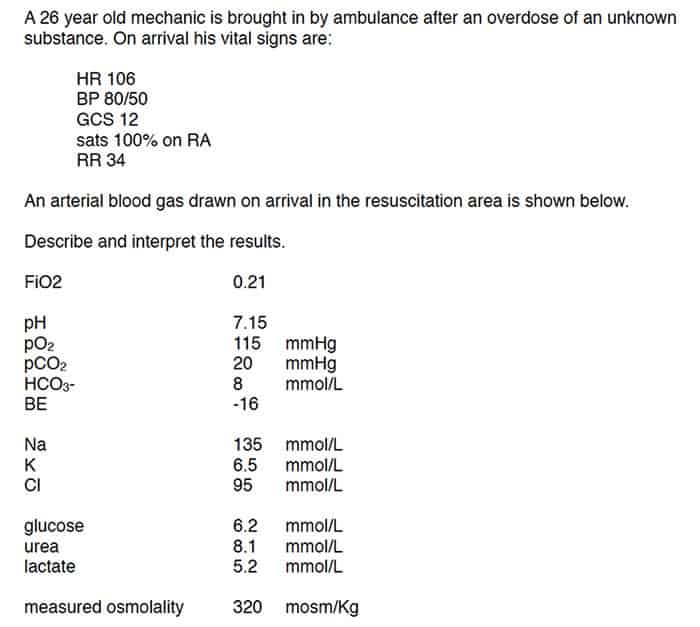
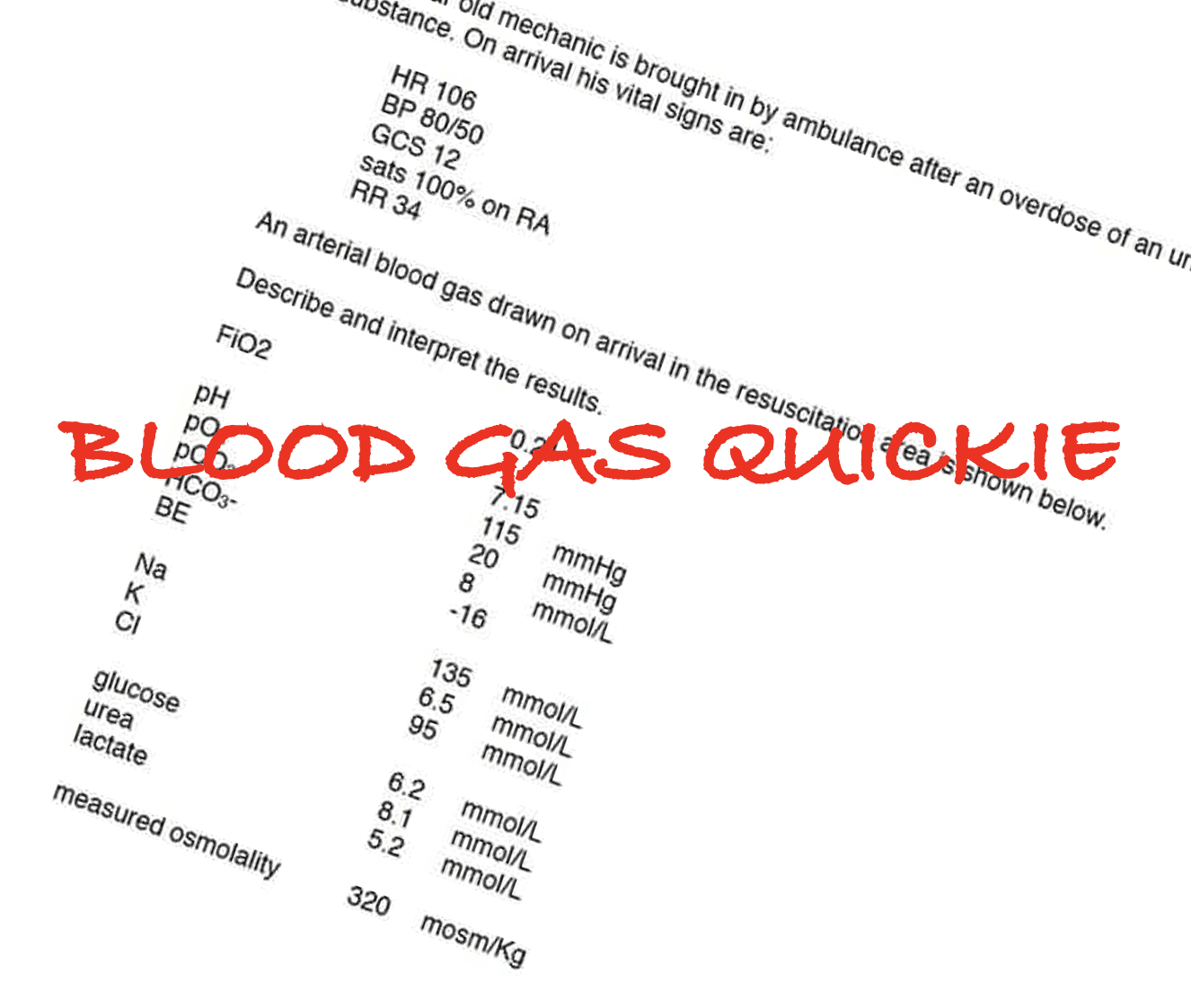
This is a question from a previous Fellowship Examination.
Without much stress, the diagnosis can be reached.
What is the diagnosis?
(a) Diabetic Ketoacidosis
(b) Lactic Acidosis
(c) Organophosphate Toxicity
(d) Ethylene Glycol Toxicity
(e) Renal Tubular Acidosis
Scroll Down…….
The key here is to be able to read the gas and make some assumptions that common sense will support.
This is a a RAISED ANION GAP METABOLIC ACIDOSIS with a RAISED OSMOLAR GAP. This suggests ETHYLENE GLYCOL OR METHANOL INTOXICATION
We will work through the above example in a moment.
The answer of course is (d)
Work through the steps to interpreting a gas
1. IS IT ACIDOSIS OR ALKALOSIS?
If the pH < 7.35 Consider Acidosis
If the pH is > 7.45 Consider Alkalosis
WHAT IS THE MAJOR DISTURBANCE? IS IT METABOLIC OR RESPIRATORY?
The major disturbance is reflected by the way the HCO3 or CO2 moves. It must move in the same direction as the pH.
In the above example the pH =7.15. So it is an ACIDOSIS
What is the primary disturbance? pCO2 = 20, HCO3 =8. A drop in HCO3 causes acidosis. A drop in pCO2 decreases acid(Co2 is acidic). Therefore the major disturbance is METABOLIC
METABOLIC ACIDOSIS
2.CORRECT THE DEPENDENT VARIABLE: IS THERE COMPENSATION?
If metabolic- correct CO2, If Respiratory correct HCO3
Given that this is a METABOLIC ACIDOSIS, we need to use the HCO3 to correct the pCO2.
The expected pCO2 is 1.5xHCO3+8 = (1.5 x 8) + 8 = 24
The actual CO2 is 20. That is vey close. We can say that there may be a respiratory alkalosis, however I would say compensation has occurred.If this was a RESPIRATORY Driven issue, where the acidosis or alkalosis, was due to the CO2, then we would need to correct the HCO3 using the CO2.
Example of a respiratory cause:
A 65 yo male presents to the emergency department with SOB. His ABG is:
pH 7.16
PCO2 68
HCO3 28
How do we interpret this?
1. It is an ACIDOSIS
The primary disturbance is: Respiratory as the pCO2 is high. It is a RESPIRATORY ACIDOSIS
2 BECAUSE IT IS A RESPIRATORY ACIDOSIS, we need to correct the HCO3.
The COs is 68 ie., 48mmHg more than 40(baseline)
In ACUTE respiratory acidosis the HCO3 would rise by 1 mol/L for every 10mmHg rise above 40. i.e. 4.8 x 1 = 4.8
The baseline of Bicarb we use is 24. You would expect the bicarb to be 28.8. It is 28…close enough
3. CALCULATE THE ANION GAP AND DELTA RATIO
THE ANION GAP is Na-Cl-HCO3 and should be equal to 12. A HIGH Anion Gap by definition must mean that a Metabolic Acidosis is present.
The DELTA RATIO allows us to look for mixed disturbances as well as to pick up Metabolic Alkalosis.
Delta Ratio = [Change in AG/ change in HCO3] = AG- 12
24-HCO3
What is the Ratio?
<0.4 = Normal Anion Gap Metabolic Acidosis (NAGMA)
0.4-0.8 = NAGMA + RAGMA(Raised Anion Gap Metabolic Acidosis)
1 = RAGMA
2 = There is a concurrent metabolic alkalosis
The ANION GAP for the case above is: 135-95-8 = 32- There is a raised anion gap.
The causes of a raised anion gap metabolic acidosis are several. We often use the mnemonic CATMUDPILES:
C: Cyanide, carbon monoxide
A: Alcoholic Ketoacidosis
T: Toluene
M: methanol, metformin
U: Uraemia
D: DKA
P: Paraldehyde, Paracetamol
I: Iron, isoniazid
L: Lactic acid
E; Ethylene glycole
S: Salicylates
The DELTA Ratio is 32-12 / 24-8 = 20/16 = 1.25
4.CALCULATE THE OXYGENATION
A-a gradient: A-a = [(760-vapour pressure) x FiO2 – 1.25 x PaCO2] – PaO2
At FiO2 of 21% ie room air (760-47) x .21 = 150
You can estimate the others
–At 40% ~ 300mmHg
-At 60% ~ 450mmHg
IF ELEVATED A-a GRADIENT, What might be the causes? Think of the Following:
–APO
–ARDS
–PE
–LRTI
–Other resp disease
A-a = 150-(1.25×20) -115 = 150-25-115=10
Expected is age/4 i.e. 26/4=6. Slightly raised.
5.LOOK AT ALL THE ELECTROLYTES:
Na –correct for gluc Na + (Gluc-5)/3
K – For each 0.1 pH fall below 7.4 the K should rise by 0.5mmol/l above 5
U:C ratio
Osmolality 2Na + U + Glc
Large osmolar gap = methanol, ethylene glycol
Picture
Na: is 135
K: the pH is 7.15 i.e. .25 below 7.4. Therefore expect K to be 2.5 x 0.5 above 5mmol/L ie., 6.25. The actual K is 6.5.
U:C ratio- make sure both are in the same units. In this case creatinine is not given
OSMOLAR GAP
The osmolar gap is useful for trying to identify osmotically active toxins (alcohols and others)
Does not detect small amounts of toxic alcohols
Does not detect late presentations – dangerous active metabolites present but not osmotic.
Calculated Osmolarity =2xNa + urea + glucose [ + EtOh ] Usually 270-290mmol/L normal range.
Osmolar gap = osmolality – calc osm [ n<10]
Large gap implies presence of an osmotically active unmeasured compound. Multiply by (molecular weight/10) for the mg/dL
Osmolality = 2×135 + 8.1+6.2 = 284.3. The measured osmolality is 320mosm/kg, so an osmolar gap of 36. This is large- one thing causes this: a toxic alcohol.
Interpretation of the Case
This is a raised anion gap metabolic acidosis, with respiratory compensation and a large osmolar gap. The cause is a toxic alcohol
The 5 Possibilities:
The ABG or VBG will have certain abnormalities. At most 3 abnormalities. We must know the potential causes of these.
1 METABOLIC ACIDOSIS- HIGH ANION GAP
We have already covered this. The causes are CATMUDPILES
2 METABOLIC ACIDOSIS- NORMAL ANION GAP: ABC
This occurs as the loss of HCO3 is replaced by Chloride, thus the anion gap stays constant, however there is a hyperchloraemic acidosis. I remember the causes as anything that decreases bicarb (HCO3) or increases Chloride:
- Bicarb loss:
- GIT Losses as in diarrhoea
- Renal Tubular Acidosis
- Drugs that stop the reabsorption of HCO3
- 85% of HCO3 is reabsorbed in the pro tubule and 15% in the rest of the tubule. Acetazolamide stops proximal tubular reabsorption of HCO3
- Addition of Chloride
- As fluid
- As acid: CaCl, NH4Cl
- Addison’s Disease: Adrenal insufficiency due to adrenal failure; look for low Na and high K(not always there)
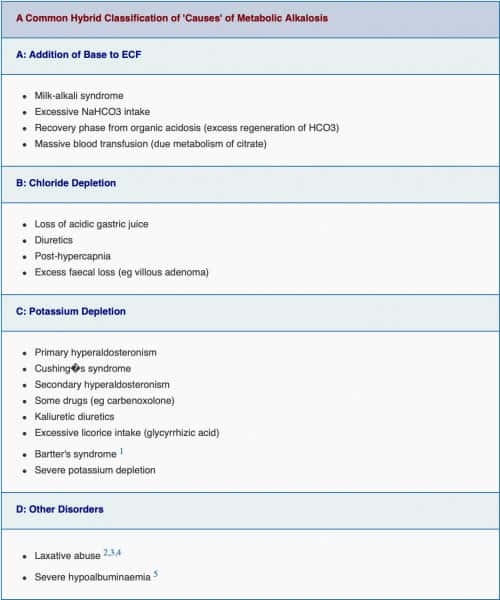
3 METABOLIC ALKALOSIS
When the bicarbonate rises above 24mmol/l, the kidney rapidly excretes it. If you give IV HCO3, there is a transient rise in HCO3 in the plasma, then the kidney excretes it.
This has been called the ‘waterfall effect’. You fill a bucket with water and no water is lost, however after the bucket is full, all the excess water spills over the side. This is the way the kidneys behave with HCO3.
So metabolic acidosis is due to:
- increased addition of HCO3
- Loss of acid- from the kidney or the gut
The maintenance of the disorder is due to one of two major factors:
- Chloride depletion- they need chloride to correct
- Loss of Gastric acid secondary to vomiting
- Diuretics: frusemide and thiazides interfere with reabsorption of Cl and Na
- Potassium depletion is due to mineralcorticoid excess. Potassium depletion results in increased bicarbonate reabsorption.
4 RESPIRATORY ACIDOSIS
Most cases are due to decreased ventilation.
This may be due to lung damage, nerve or muscle disorder, or depressed conscious state.
5 RESPIRATORY ALKALOSIS
This is due to hyperventilation. This can be due to pulmonary causes such as airways disease(asthma) or PE, or central causes, such as stroke, head injury, pregnancy or related to drugs such as salicylate.





What i do not understood is actually how you’re not actually a lot more neatly-liked than you may be right now.
You are so intelligent. You recognize therefore significantly relating to this subject, produced me
personally imagine it from so many numerous angles. Its like women and men aren’t interested unless it’s one thing to accomplish with Woman gaga!
Your own stuffs great. Always deal with it up!
Hi! I just wanted to ask if you ever have any issues with
hackers? My last blog (wordpress) was hacked and I ended up losing months of hard work due to no back up.
Do you have any methods to stop hackers?
This design is steller! You certainly know how to keep a reader entertained.
Between your wit and your videos, I was almost moved to start my own blog (well, almost…HaHa!) Fantastic job.
I really enjoyed what you had to say, and more than that, how you presented it.
Too cool!