A 29 yo female presents with tachycardia and shortness of breath and some pleuritic chest pain. She has driven from interstate for the last 8 hours.
Examination reveals vitals of:
- Heart rate of 108bpm sinus
- BP 105/68
- Saturations of 87% on room air
The physical examination is normal.
The working diagnosis is a pulmonary embolism.
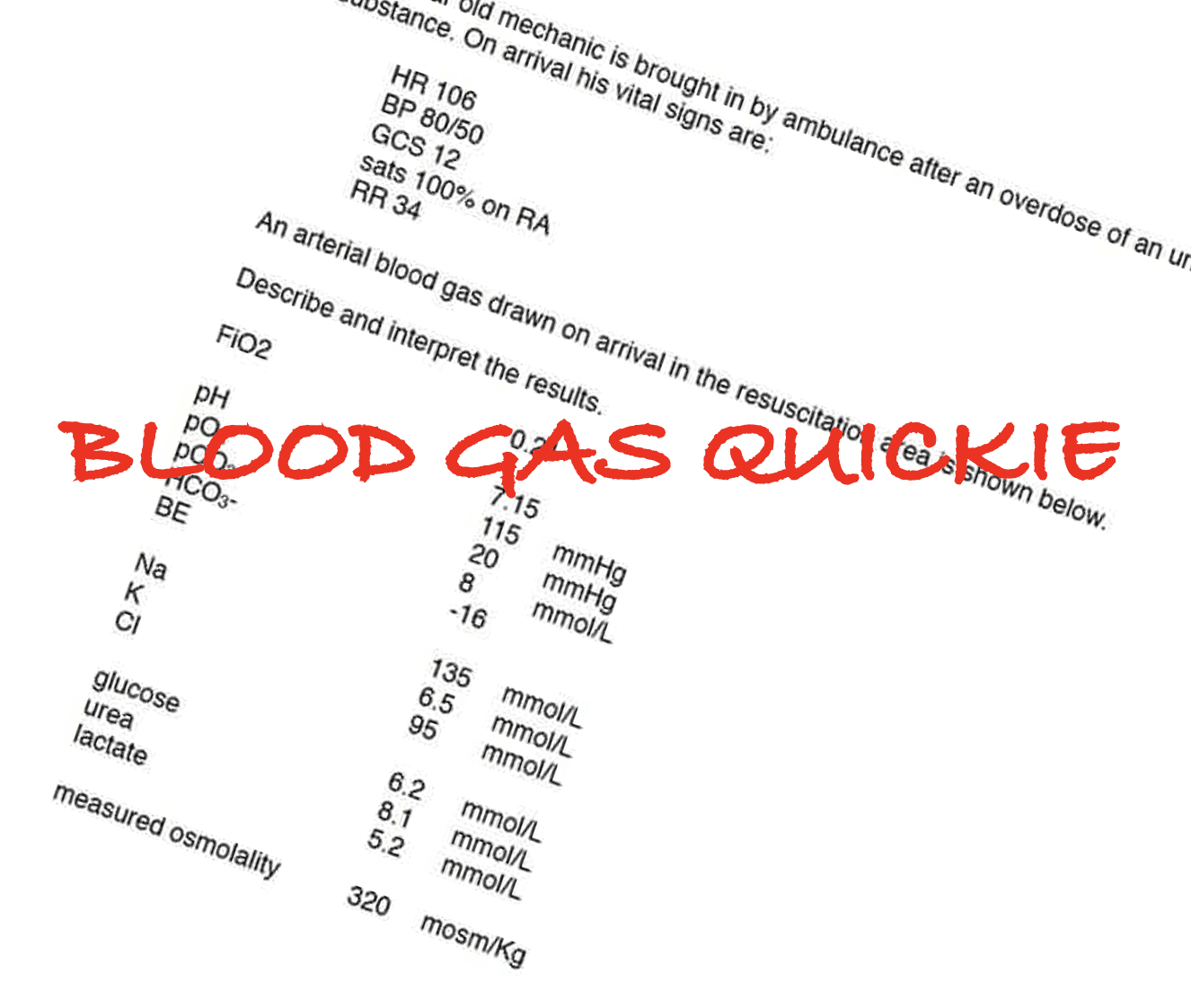
The patient is seen in a resuscitation cubicle, placed on oxygen, an IV canula inserted and bloods are done, including a blood gas. The blood gas shows the following:
- pH 7.01
- CO2 67
- O2 68
- HCO3 11
Interpretation of the blood gas (refer to Reading the ABG):
This is a primary RESPIRATORY ACIDOSIS. If in doubt always look at the CO2- it determines if an acidosis is respiratory or metabolic in origin. With a CO2 of 67 what would we expect the HCO3 to be?
For an acute insult, the HCO3 increases by 1 mmol/L for every 10mmol increase in CO2 above 40:
HCO3 = 24+1(HCO3-40/10) = 24 + 1(67-40/10) = expected HCO3 is 26.7
We can look at what it should be in chronic respiratory acidosis, however the patient does not have any history of chronic respiratory illness, so it is an academic exercise. If we did calculate it we would expect that the CO2 will increase by 4mmol/L for every 10mmol increase in CO2 above 40 ie we would expect the CO2 to be 24+4(67-40/10) = 34.8. Our CO2 is much higher than this.
You notice that when the nurse attached the oxygen via nasal prongs she used an ETCO2 cannula to do so, to measure the respiratory rate. The ETCO2 is reading 32.
Why is there such a difference between the ETCO2 and PaCO2?
There is a Ventilation/Perfusion mismatch. There is pulmonary vasoconstriction, so no CO2 diffusing from the circulation into the alveoli. This is why the ETCO2 is lower than the PaCO2. The CO2 is simply not entering the lungs.
Does putting the patient on CPAP help?
Does putting the patient on high flow oxygen help?
Does intubating the patient and increasing the respiratory rate help?
The answer is NO to all of these. You can’t blow off or wash out what isn’t getting in there. None of these things will help until the pulmonary vascular constriction is dealt with.
What if we gave NaHCO3? Surely this would fix the acidosis. This is what it might look like after giving it:
- pH 7.07
- PaCO2 92
- PaO2 68
- HCO3 22
The CO2 has risen even further with a slight rise in the HCO3. This is because Bicarb turns into H20 + CO2, increasing the PaCO2, however the ETCO2 will be the same, as there is no perfusion of this CO2 into the lungs.
Think about this next time you see a pulmonary embolism patient and the CO2 isn’t making any sense.







Hypoxia vasoconstriction will be improved by administering O2 and therefore will reduce dead space ventilation and reduce pA CO2