Ketamine-only breathing intubation(KOBI), is a technique where Ketamine(+/- topical local anaesthetic) is used to facilitate intubation in patients that may not be able to tolerate traditional Rapid Sequence Intubation(RSI)
3 Approaches to Ketamine use in intubation
- Ketamine as the induction agent in normal RSI: It shows haemodynamic stability and a long duration of action
- Ketamine in Delayed Sequence intubation: It facilitates pre-oxygenation in the un-cooperative patient. Dosages of 1-2mg/kg IV can be used. When pre-oxygenation has been achieved, a paralytic agent can then be used, as in traditional RSI.
- Ketamine as the dissociative agent, with or without topical anaesthetic. An example of its use here, is in the patient exposed to a fire, that has carbonatious sputum. An airway needs to be established, but there is concern about the state of swelling in the airway. Ketamine is used to control the patient, whilst the cords are viewed, preferably by video laryngoscopy. See this case with images below. There are other indications for it.
What is Ketamine-only breathing intubation(KOBI)…and why would we use it?
Ketamine in a dissociative dose of 1-2mg/kg IV has both an amnesic effect and dampens the effect of painful stimuli. At this same time the airway reflexes are maintained. We don’t call it awake intubation as we might with a topical anaesthetic-only approach, as the patient is not awake.
Merelman et al(1) describe 4 situations where the patient can benefit from KOBI:
- Patients with a high oxygen deficit, where even a short duration of apnoea, can have dire consequences. This is classically your patient with pneumonia or ARDS, where aggressive oxygenation attempts with mask or NIV cannot get the saturations up above 95%.
- In traditional RSI, that time after paralytics where apnoea occurs and no oxygen is being delivered, can result in cardiac arrest.
- Apnoeic oxygenation is usually of no great benefit in these patients.
- There are techniques for using traditional RSI in these situations, however Ketamine may be an alternative.
- (In deep sedation, Ketamine will reduce minute ventilation, but that is preferred to apnoea.)
- In patients where awake intubation would normally be required, but due to lack of skills or time etc, this approach cannot be used.
- In the acidotic patient with high minute ventilation (DKA, toxic alcohol, lactic acidosis). Using spontaneous respiration may be a way of decreasing the risk associated with peri-intubation decompensation.
- These are the patients that will have sudden cardiac arrest on intubation with traditional RSI.
- The hypotensive patient. Although Merelman(1) discusses this type of patient, the approach would be to resuscitate aggressively BEFORE and intubation attempt is made, so that the chance of hypotension is reduced.
- In traditional RSI, when the patient becomes apnoeic and then transitions from negative to positive pressure, there is a decreased in venous return leading to potential cardiovascular collapse.
What can make Ketamine-only intubation difficult?
MUSCLE RIGIDITY: This can occur with Ketamine. The solution is to give Midazolam, but this can then cause hypotension etc..
LARYNGOSPASM: This certainly has been shown to occur with Ketamine. Some PEEP may assist, however in most cases paralytics will be needed. The problem here will be that this patient with high oxygen requirements has now gone into laryngospasm and then needs to wait for the paralytic to work. Not a good scenario.
VOMITING: Airway reflexes are not totally abolished, so it may lead to coughing and gagging.
An example where it can be used
A patient is brought into the ED after being rescued from a house fire. He has no visible burns, but his nasal hairs and eyebrows are singed and he has carbonaceous sputum. His voice sounds altered(although we aren’t sure), so we are concerned about potential airway swelling. The carbonaceous sputum is an indication for early intubation, but we are not sure of the state of the airway and how difficult intubation might be. We used Ketamine and topical anaesthetic with video laryngoscopy, as a means of visualisation and to facilitate intubation.
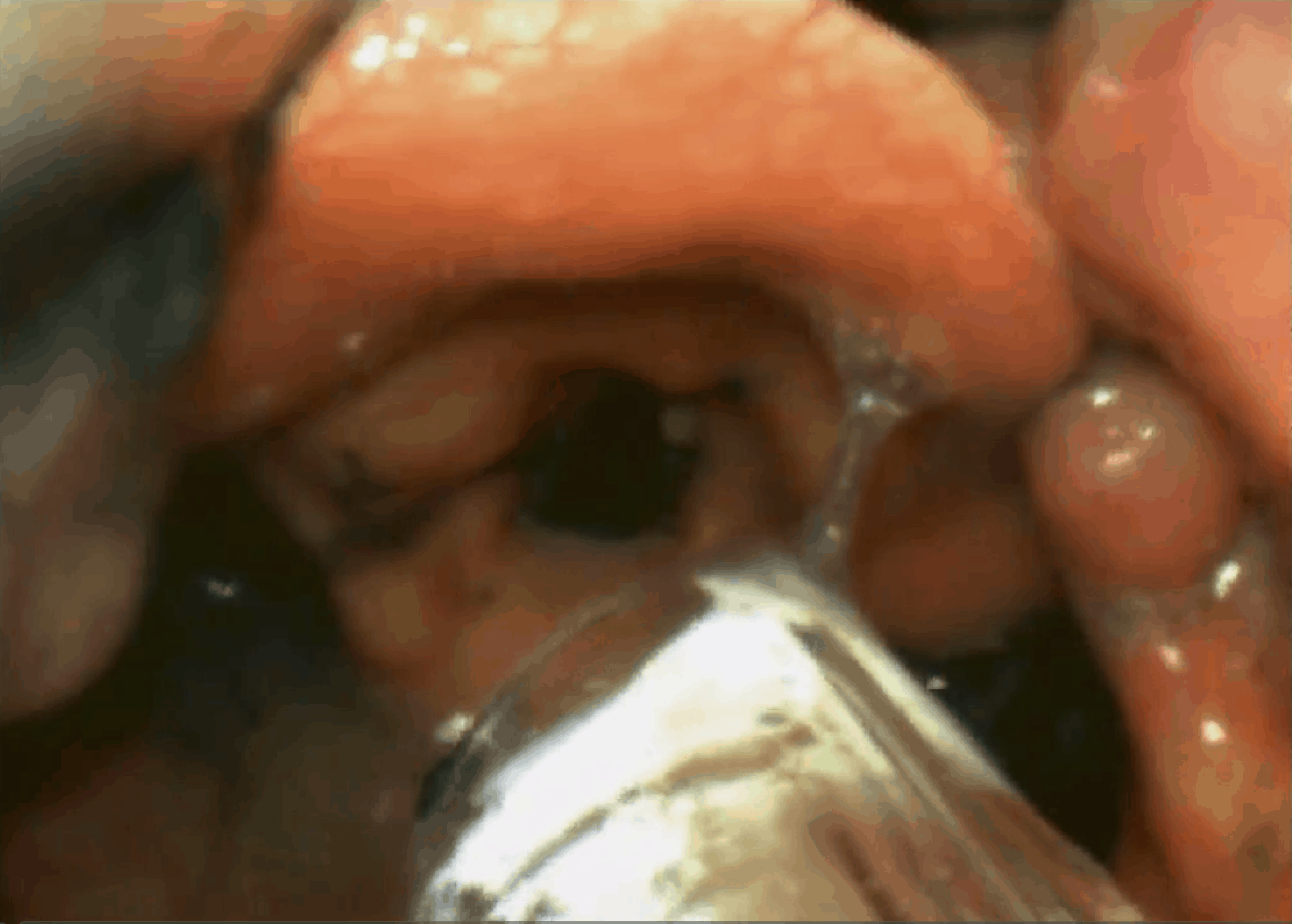
Ketamine is used to sedate/dissociate the patient (1mg/kg IV). Atomised local anaesthetic is used on the airway to dampen the gag response and allow us to progressively get a better look. The airway is suctioned and although the cords are seen to be slightly swollen, intubation is certainly possible. The patient has been breathing spontaneously this whole time. A paralytic agent is given and the tube is passed under direct vision. The tube might also have been passed, under direct vision, with no paralytic agent, however to avoid laryngospasm and any other complications it was decided to paralyse the patient. See the images below.
-


Atomised local anaesthetic is used. Carbon deposits seen -
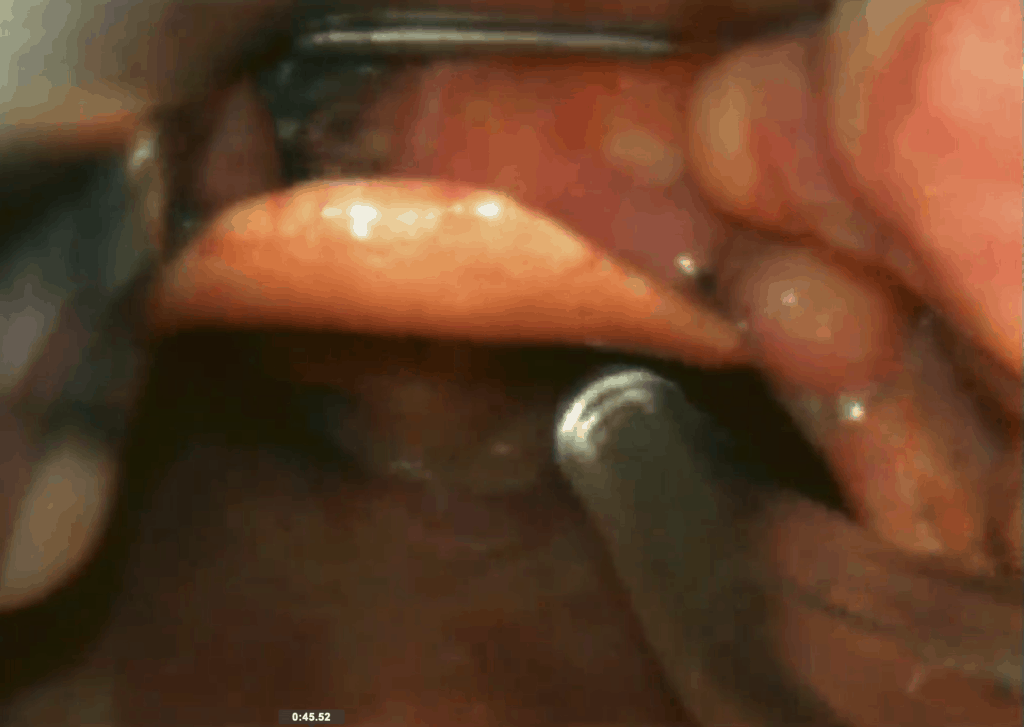
The airway is suctioned. Patient is tolerating this well -


Cords are viewed and ETT is ready to go -

Paralytic agent is given and the ETT is passed under direct vision.
References
- Merelman A et al. Alternatives to Rapid Sequence Intubation: Contemporary Airway Management with Ketamine. West J Emerg Med 2019;20(3):466-471







What’s up mates, its enormous paragraph regarding teachingand
completely explained, keep it up all the time.
Thank you for the auspicious writeup. It in fact was a enjoyment account it.
Glance complex to more delivered agreeable from you! However, how can we keep in touch?
Hello, everything is going perfectly here and ofcourse every
one is sharing information, that’s in fact fine, keep up writing.
Howdy! Do you use Twitter? I’d like to follow you if that would be okay.
I’m definitely enjoying your blog and look forward to new posts.
Its such as you learn my mind! You seem to grasp a lot approximately this, such as you wrote the
book in it or something. I feel that you simply can do with a few percent to force the message house a bit, but other than that, this is great blog.
A fantastic read. I will certainly be back.
I loved as much as you’ll receive carried out right here. The sketch is tasteful, your authored material stylish. nonetheless, you command get bought an impatience over that you wish be delivering the following. unwell unquestionably come further formerly again since exactly the same nearly a lot often inside case you shield this hike.