An interview with a world expert.
Earlier this year I postponed the Singapore EMCORE Conference, due to COVID-19, but only after a lot of serious thought. The decision was the right one. We are now seeing the effects. With what would have been only 3 weeks away from that conference, conference leave is being cancelled all over the country and travel insurance companies will no longer refund, due to COVID-19.
There’s a lot of fear out there about this virus (rightly so) and there are some huge gaps in knowledge and a lot of misinformation, especially about it’s spread outside China.
We continuously talk about it as being a ‘cold’, one of many Corona Viruses, but I think that many have missed the point. That is, it may not affect us personally in a severe way if we are young and healthy, but if we think of the most vulnerable in our population, the potential downside is very disturbing.
I asked Ian Norton (ex WHO) a few questions.
I got to ask Ian Norton about what’s happening and posed a couple of questions, from which came these responses. I will edit it below for you. Compelling reading.
A few words about who Ian is.
From 2014- 2020 Ian worked with the World Health Organization (WHO) setting up and running the Emergency Medical Team (EMT) Initiative program in HQ Geneva. He wrote the international standards for EMT responses in disasters, outbreaks and conflicts. With WHO he deployed for over 5 months to West Africa as part of the Ebola outbreak response in 2014/15 and led the coordination of 60 EMTs in three countries. He also led the coordination of 132 EMTs in Nepal during the earthquakes of April and May 2015…. and it goes on. I am eagerly waiting to hear him speak at EMCORE Sydney.
Here’s the discussion:
Peter: Although we see a lot of medicos downplaying this situation, it has significant repercussions given the prediction of a 40-70% worldwide infection rate. It may not be a threat to younger well people, but the very high infection load will have a downstream effect on those that are more vulnerable and that will be very significant. Yours views?
Ian: This is a really significant outbreak. I’m really worried by several aspects of this outbreak.
It’s fast, with a reproductive rate of 2.5 ie., every person infects 2.5 others without containment measures and there is evidence of super spreaders and those who feel well with active disease making them a classic “typhoid Mary”….. she thought she was well!
The impact on the elderly and previously unwell is really significant and in an ageing population like ours and other Western countries the impact will be huge. I’m personally worried about the effect on my own parents and people I know…. It’s disappointing that everyone seems panicked about themselves, we should all be redoubling our efforts to protect our most vulnerable, not ourselves.
I’m worried about the worried well, overwhelming our clinics and ED’s, and I’m worried about the overall effect on the health system of this level of demand. I always struggled to get the WHO and epidemiologists to understand that in clinical care the number of confirmed is only a part of the story, the real burden is the number of people who seek care, not only those who eventually turn out to be positive. If we were to track the number of presentations of suspect cases (plus confirmed) that’s an excellent indicator. In Ebola just last week in DRC (where the outbreak is finally ending) there were over 5,000 people traced and investigated each day… even though the case number is zero and has been for weeks… that’s the real work. For ED’s we all know it’s the number who present we count, not the number who have disease x or y.
The down stream effect of this is catastrophic on access to healthcare. In Ebola in West Africa in 2014/15 11,000 people may have died of the disease but well over 33,000 died through lack of access to healthcare to treat their malaria, diarrhea, cancer or injury etc. (Karolinska Institute study 2015). In Australia, New Zealand and the Pacific we will not just be counting the burden of Coronavirus mortality, but the numbers of people who will die or suffer worsening morbidity because they cant see their GP or get access to their outpatient clinic or surgery.
I’m worried that sometimes the people who write the best technical documents and plans and sit in key management positions, are not best placed to operationalize them in crisis. The skill sets to write good documents are not always the skills sets you need for adaptive and flexible thinking in scale ups like this….. I faced exactly these issues in the recent Earthquakes and outbreaks I helped coordinate with the WHO and I’m seeing signs of it now…. We do need to take those 400 page technical documents and now make them 1 pagers, flow diagrams and provide practical operational advice that works at the clinic and ED level. We only have a few more weeks before it will be too late for preparation anymore and we are fire-fighting.
I’m also disappointed but can see the reasoning, behind countries starting to look after themselves, hold on to stock if it’s made domestically, all things that the richest countries swore they wouldn’t do at various global meetings on this ( I clearly remember this on the topic list at Davos world economic forums, the G7 and G20 meetings etc… all hot air)…. Good intentions in peace time have been thrown out in some cases, and if we don’t look after each other now we will all be worse off. This is one of those times were “Coordination saves lives” but there is a vacuum at the global level in this area.
Peter: The large urban centres are equiped with tests and isolation rooms etc. I work in a rural setting, as many doctors do in Australia. If I isolate all presenters that are well in their own homes, we lose a significant amount of the workforce and our towns are paralysed. Should I be testing well all-comers and self isolating them and then being able to clear them within 24 hours(72 hours in reality)? What are your views on the impact as we go forward, especially entering the winter months?
Ian: I agree urban and rural areas will be hard hit, but perhaps in different ways. The key will be good access to lab tests early, but this will fade quickly as the numbers grow… ask yourself why do you need the test (that’s what I love telling the medical registrars when they used to ask me to do x or y test in ED…. Why are you doing it?)…. For this coronavirus we will halt testing with sustained community transmission, it won’t matter soon, and you will be freer to presume diagnosis and treat on symptoms.
I had a conversation with colleagues still in WHO and leading this response just two days ago…. They do not yet have a good predictive scoring system, but we need one quickly. We need to arm everyone in the frontline clinical positions with the right flow plans to see and reassure, see and treat and send home with clear instructions when to come back, and we need good clinical predictive scores to decide who needs to come in and use the very scarce resources we have. The lessons we learned in every recent response to truly huge outbreaks is that if high level intervention isn’t useful, or there isn’t a therapeutic past general support, then people will want to stay local, and so will want to be treated in the local hospital.
I’m not sure what Australians will want, but if they knew the conditions in the big ICU’s at the height of something like this, they may want to stay local too. We have to have some difficult conversations on palliation and resource management of ventilators and oxygen supplies now, and lets not just have a quiet conversation among a few “experts” that doesn’t involve multi-disciplinary staff, patients and carers…. Everyone needs to know how bad it could get and the tough choices that be ahead of us.
OKAY that’s all I’ve got for now.
We need to talk about scoring systems and also address the issue of the paediatric population. Kids aren’t protected. What they are is carriers. What’s the impact of snuffly kids coming to us especially in the upcoming winter months?
Our hospital for one, has commenced discussions with everyone in the region. The Wimmera covers about 30,000sqkm and we are the emergency department. When the height of this hits, which by my reckoning, will be late June, we will have to ask the difficult questions.
I’ll keep you updated when I get more.
For some sites to visit:
Johns Hopkins Centre for Health Security produces a daily recap on this situation.
The WHO obviously has a summary.
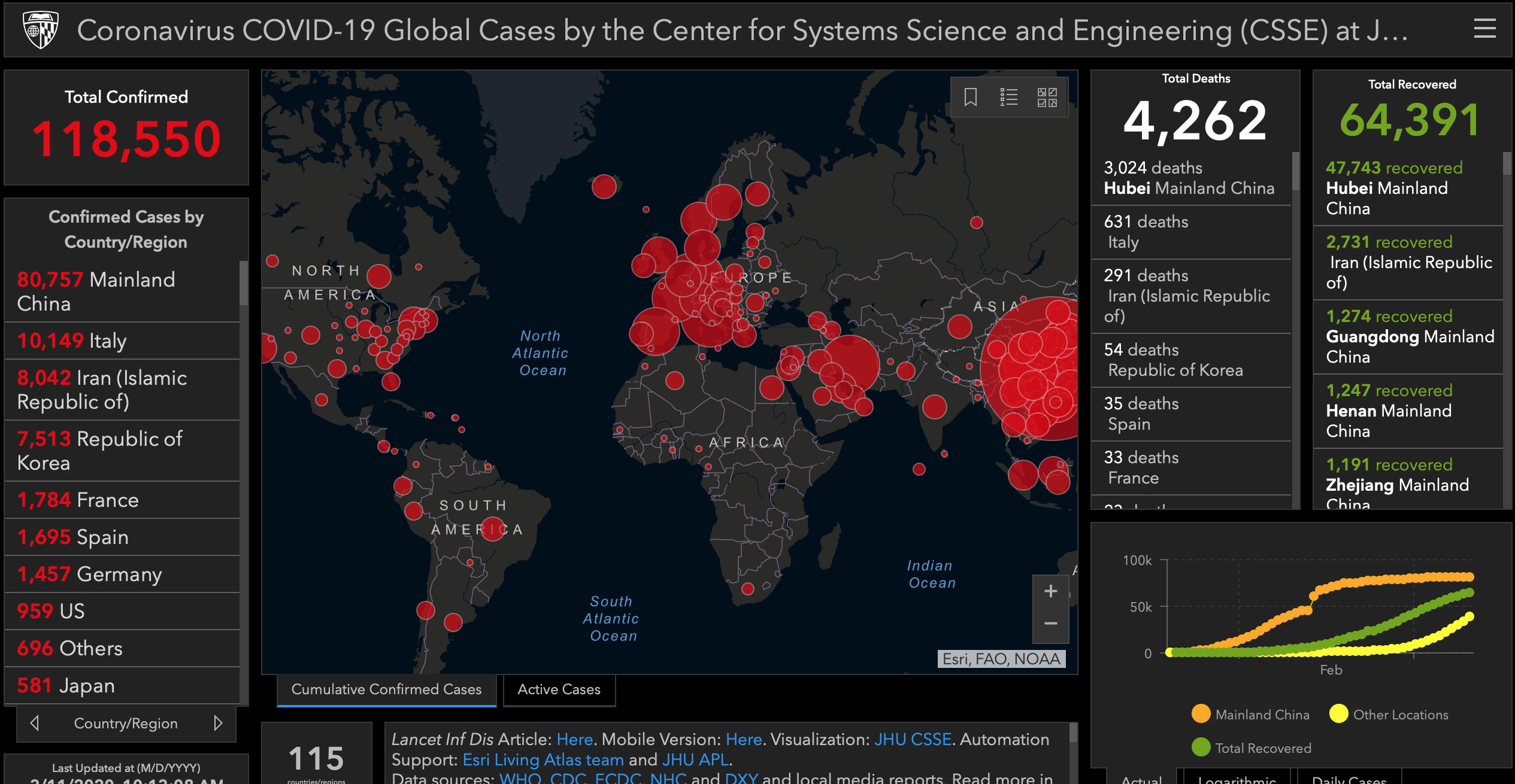
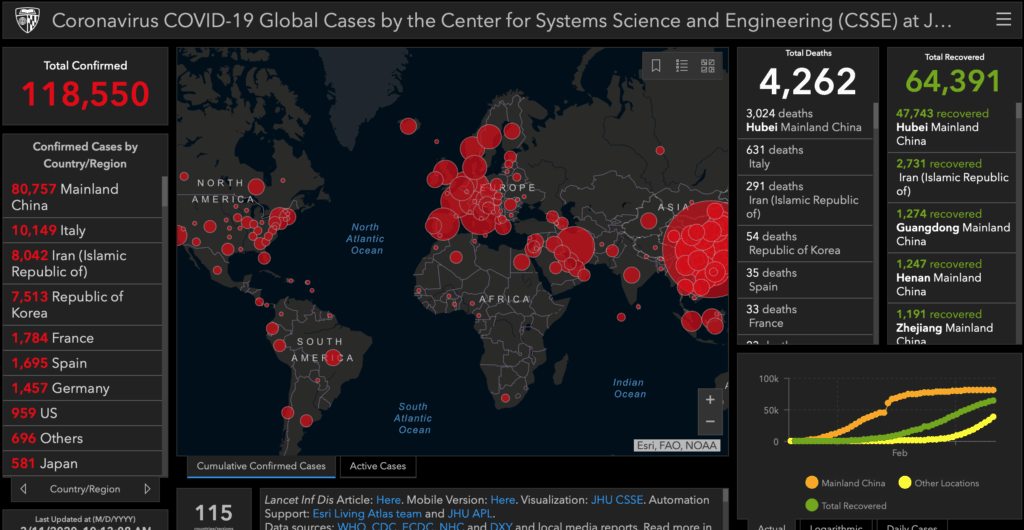
Below is a heat map as of 11/03/2020 (Source: Johns Hopkins of the latest numbers- Find it Here.)







COVID-19: Interview with a world expert – Resus
argfcndnmlc
[url=http://www.g6b0lx3v3x14fvij344097oz48eew57hs.org/]urgfcndnmlc[/url]
rgfcndnmlc http://www.g6b0lx3v3x14fvij344097oz48eew57hs.org/
Kids Custom Umbrella
ブランドバッグコピー
Anavar 50
ブランドコピーRolexロレックスN級品
StellaMcCartneyステラマッカートニーバッグコピー
Canned Pineapple
最新ブランドスーパーコピー代引き
Cool Sports Bras
3 Point Hitch Seeder
SaintLaurentサンローラン靴コピー
Hermesエルメスブレスレットスーパーコピー
Intelligent Speaker Mesh
portaloo camping
DIORディオール指輪コピー
Puffco Peak Pro review: This pricey portable dab rig is worth it ? GEEKSPIN
Diorディオール帽子販売店
Barium Hydroxide Monohydrate
スーパーコピーバッグ
Chanelシャネルブレスレット販売店
Alcohol Cleansing Wipes
Locking Key Cabinet
ブランドコピー代引き
ブランドGucciグッチイヤリングコピー代引き
Led Drop Ceiling Lights
A106 Gr.B Seamless Pipe
ChristianLouboutinクリスチャンルブタン靴販売店
Lightweight Glasses
ブランド時計コピー
コピー時計
Coupling Alignment With Dial Indicator
ブランドコピー専門店
Automated Rna Extractor
ブランドコピー専門店
Agricultural Silicone Additive
ブランドコピー専門店
Horizontal Conveyor
Camshaft Position
Bulk Bags With Discharge Spout
ブランド財布コピー
06A906031CE
Steel
スーパーコピーブランド
20T Round Cooling Tower